

Defining local-regional control and its importance in locally advanced non-small cell lung carcinoma
- PMID: 22425920
- PMCID: PMC3335930
- DOI: 10.1097/JTO.0b013e3182429682
Defining local-regional control and its importance in locally advanced non-small cell lung carcinoma
Abstract
Introduction: Local-regional control (LRC) rates for non-small cell lung cancer after chemoradiotherapy were studied (using two different definitions of LRC) for the association between LRC and survival.
Methods: Seven legacy Radiation Therapy Ooncology Group trials of chemoradiotherapy for locally advanced non-small cell lung cancer were analyzed. Two different definitions of LRC were studied: (1) freedom from local progression (FFLP-LRC), the traditional Radiation Therapy Oncology Group methodology, in which a failure is intrathoracic tumor progression by World Health Oorganization criteria; and (2) response-mandatory (strict-LRC), in which any patient not achieving at least partial response was considered to have failure at day 0. Testing for associations between LRC and survival was performed using a Cox multivariate model that included other potential predictive factors.
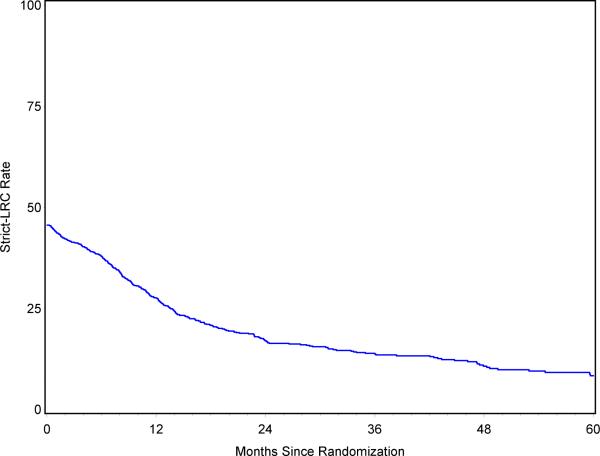
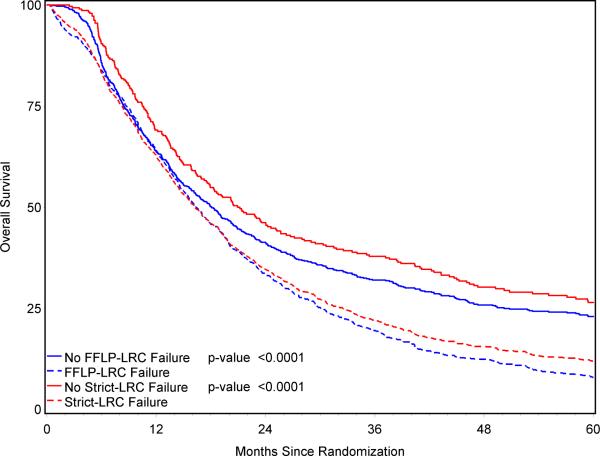
Results: A total of 1390 patients were analyzed. The LRC rate at 3 years was 38% based on the FFLP-LRC definition and 14% based on the strict-LRC definition. Performance status, concurrent chemotherapy, and radiotherapy dose intensity (biologically equivalent dose) were associated with better LRC (using either definition). With the strict-LRC definition (but not FFLP-LRC), age was also important. There was a powerful association between LRC and overall survival (p, 0.0001) on univariate and multivariate analyses. Age, performance status, chemotherapy sequencing, and biologically equivalent dose were also significantly associated with survival. Histology and gender were also significant if the strict-LRC model was used.
Conclusions: LRC is associated with survival. The definition of LRC affects the results of these analyses. A consensus definition of LRC, incorporating functional imaging and/or central review, is needed, with the possibility of using LRC as a surrogate end point in future trials.
Figures

References
-
- Perez CA, Bauer M, Edelstein S, Gillespie BW, Birch R. Impact o ftumor control on survival in carcinoma of the lung treated with irradiation. Int J Radiat Oncol Biol Phys. 1986 Apr;12(4):539–47. PMID 3009368. - PubMed
-
- Marino P, Preatoni A, Cantoni A. Randomized trials of radiotherapy alone versus combined chemotherapy and radiotherapy in stages IIIa and IIIb nonsmall cell lung cancer. A meta-analysis. Cancer. 1995 Aug 15;76(4):593–601. PMID 8625152. - PubMed
-
- Perez CA, Pajak TF, Rubin P, et al. Long-term observations of the patterns of failure in patients with unresectable non-oat cell carcinoma of the lung treated with definitive radiotherapy. Report by the Cancer. 1987 Jun 1;59(11):1874–81. Radiation Therapy Oncology Group. PMID 3032394. - PubMed
-
- Le Chevalier T, Arriagada R, Quoix E, et al. Radiotherapy alone versus combined chemotherapy and radiotherapy in nonresectable non-small-cell lung cancer: first analysis of a randomized trial in 353 patients. J Natl Cancer Inst. 1991 Mar 20;83(6):417–23. PMID 1847977. - PubMed
-
- Sause W, Kolesar P, Taylor S, IV, et al. Final results of phase III trial in regionally advanced unresectable non-small cell lung cancer: Radiation Therapy Oncology Group, Eastern Cooperative Oncology Group, and Southwest Oncology Group. Chest. 2000 Feb;117(2):358–64. PMID 10669675. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
