

Remote ischaemic pre- and delayed postconditioning - similar degree of cardioprotection but distinct mechanisms
- PMID: 22427438
- PMCID: PMC3470925
- DOI: 10.1113/expphysiol.2012.064923
Remote ischaemic pre- and delayed postconditioning - similar degree of cardioprotection but distinct mechanisms
Abstract
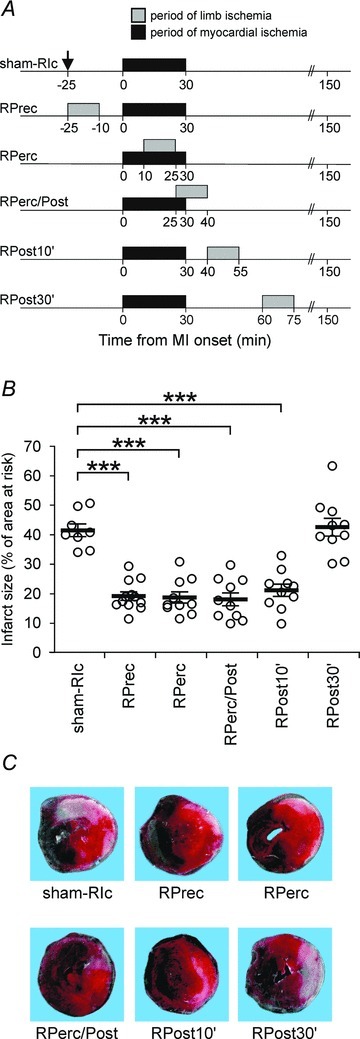
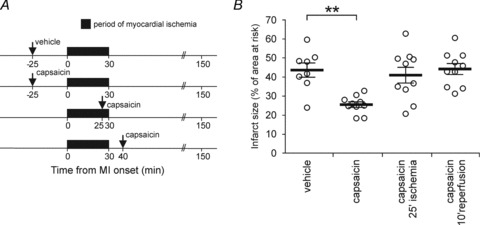
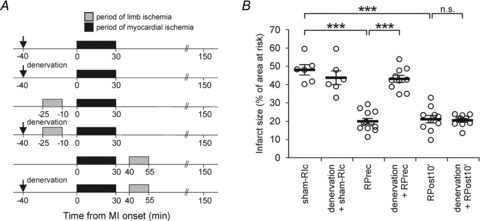
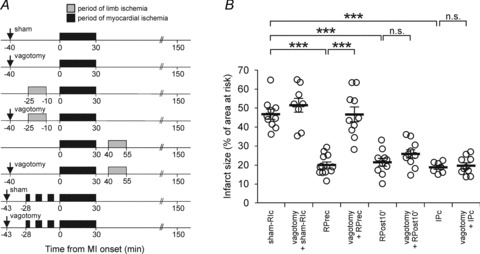
Myocardial ischaemia-reperfusion injury can be significantly reduced by an episode(s) of ischaemia-reperfusion applied prior to or during myocardial ischaemia (MI) to peripheral tissue located at a distance from the heart; this phenomenon is called remote ischaemic conditioning (RIc). Here, we compared the efficacy of RIc in protecting the heart when the RIc stimulus is applied prior to, during and at different time points after MI. A rat model of myocardial ischaemia-reperfusion injury involved 30 min of left coronary artery occlusion followed by 120 min of reperfusion. Remote ischaemic conditioning was induced by 15 min occlusion of femoral arteries and conferred a similar degree of cardioprotection when applied 25 min prior to MI, 10 or 25 min after the onset of MI, or starting 10 min after the onset of reperfusion. These RIc stimuli reduced infarct size by 54, 56, 56 and 48% (all P < 0.001), respectively. Remote ischaemic conditioning applied 30 min into the reperfusion period was ineffective. Activation of sensory nerves by application of capsaicin was effective in establishing cardioprotection only when elicited prior to MI. Vagotomy or denervation of the peripheral ischaemic tissue both completely abolished cardioprotection induced by RIc applied prior to MI. Cardioprotection conferred by delayed remote postconditioning was not affected by either vagotomy or peripheral denervation. These results indicate that RIc confers potent cardioprotection even if applied with a significant delay after the onset of myocardial reperfusion. Cardioprotection by remote preconditioning is critically dependent on afferent innervation of the remote organ and intact parasympathetic activity, while delayed remote postconditioning appears to rely on a different signalling pathway(s).
Figures
Comment in
-
Cardioprotection at a distance - remote conditioning takes the stage.Exp Physiol. 2012 Aug;97(8):905. doi: 10.1113/expphysiol.2012.067066. Exp Physiol. 2012. PMID: 22833146 No abstract available.
-
Highlights in basic autonomic neurosciences: remote ischaemic preconditioning as an autonomic reflex--a question of timing and circumstances?Auton Neurosci. 2013 Jan;173(1-2):1-2. doi: 10.1016/j.autneu.2012.11.001. Epub 2012 Nov 15. Auton Neurosci. 2013. PMID: 23159165 No abstract available.
References
-
- Argafud L, Gateau-Roesch O, Raisky O, Loufouat J, Robert D, Ovize M. Postconditioning inhibits mitochondrial permeability transition. Circulation. 2005;111:194–197. - PubMed
-
- Borutaite V, Jekabsone A, Morkuniene R, Brown GC. Inhibition of mitochondrial permeability transition prevents mitochondrial dysfunction, cytochrome c release and apoptosis induced by heart ischemia. J Mol Cell Cardiol. 2003;35:357–366. - PubMed
-
- Bøtker HE, Kharbanda R, Schmidt MR, Bøttcher M, Kaltoft AK, Terkelsen CJ, Munk K, Andersen NH, Hansen TM, Trautner S, Lassen JF, Christiansen EH, Krusell LR, Kristensen SD, Thuesen L, Nielsen SS, Rehling M, Sørensen HT, Redington AN, Nielsen TT. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet. 2010;375:727–734. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical