

Socioeconomic inequality in domains of health: results from the World Health Surveys
- PMID: 22429978
- PMCID: PMC3364884
- DOI: 10.1186/1471-2458-12-198
Socioeconomic inequality in domains of health: results from the World Health Surveys
Abstract
Background: In all countries people of lower socioeconomic status evaluate their health more poorly. Yet in reporting overall health, individuals consider multiple domains that comprise their perceived health state. Considered alone, overall measures of self-reported health mask differences in the domains of health. The aim of this study is to compare and assess socioeconomic inequalities in each of the individual health domains and in a separate measure of overall health.
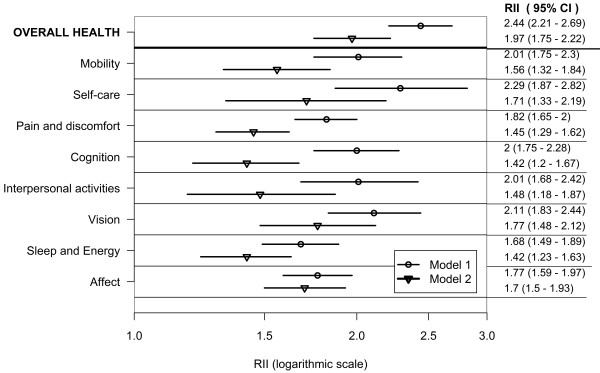
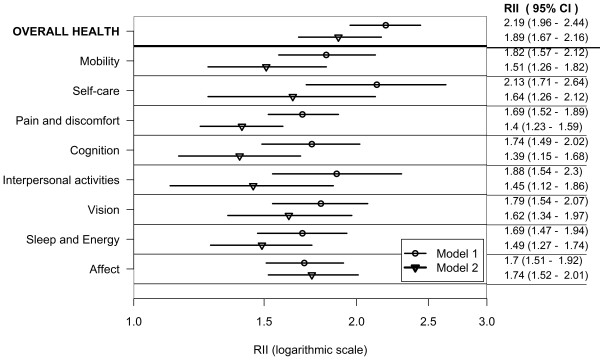
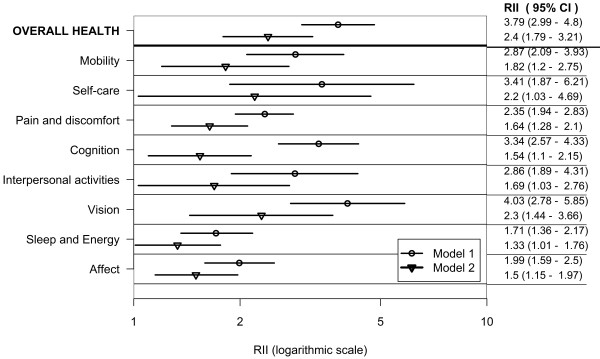
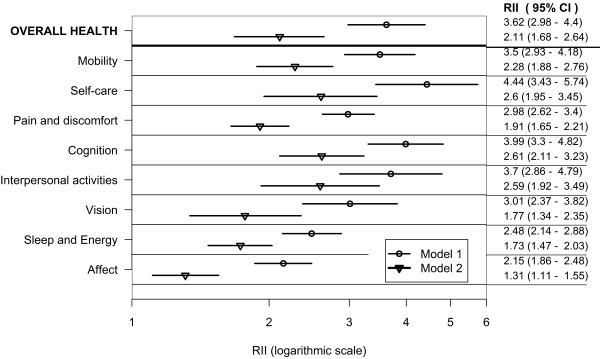
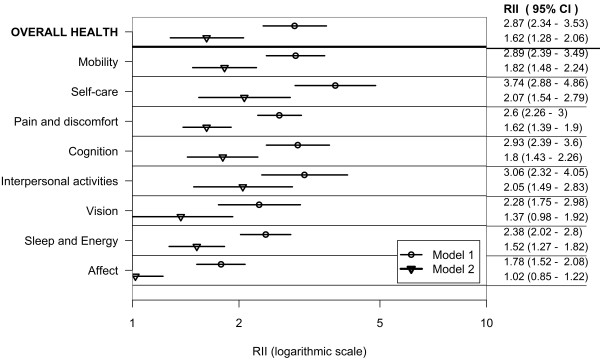
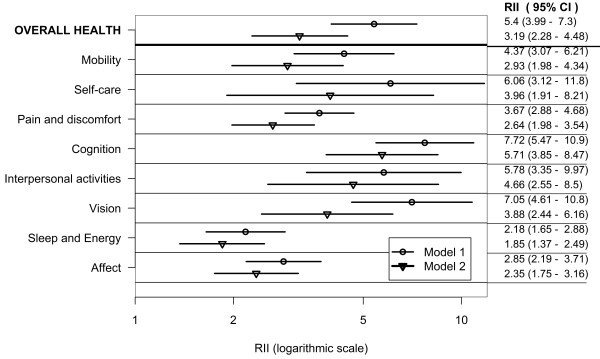
Methods: Data on 247,037 adults aged 18 or older were analyzed from 57 countries, drawn from all national income groups, participating in the World Health Survey 2002-2004. The analysis was repeated for lower- and higher-income countries. Prevalence estimates of poor self-rated health (SRH) were calculated for each domain and for overall health according to wealth quintiles and education levels. Relative socioeconomic inequalities in SRH were measured for each of the eight health domains and for overall health, according to wealth quintiles and education levels, using the relative index of inequality (RII). A RII value greater than one indicated greater prevalence of self-reported poor health among populations of lower socioeconomic status, called pro-rich inequality.
Results: There was a descending gradient in the prevalence of poor health, moving from the poorest wealth quintile to the richest, and moving from the lowest to the highest educated groups. Inequalities which favor groups who are advantaged either with respect to wealth or education, were consistently statistically significant in each of the individual domains of health, and in health overall. However the size of these inequalities differed between health domains. The prevalence of reporting poor health was higher in the lower-income country group. Relative socioeconomic inequalities in the health domains and overall health were higher in the higher-income country group than the lower-income country group.
Conclusions: Using a common measurement approach, inequalities in health, favoring the rich and the educated, were evident in overall health as well as in every health domain. Existent differences in averages and inequalities in health domains suggest that monitoring should not be limited only to overall health. This study carries important messages for policy-making in regard to tackling inequalities in specific domains of health. Targeting interventions towards individual domains of health such as mobility, self-care and vision, ought to be considered besides improving overall health.
Figures
References
-
- World Health Organization. Constitution of the WHO. Geneva: WHO; 1946.
-
- Salomon JA, Mathers C, Chatterji S, Sadana R, Üstün TB. In: Health systems performance assessment debates, methods and empiricisms. Murray CJL, Evans DB, editor. Geneva: World Health Organization; 2003. Quantifying individual levels of health definitions, concepts and measurement issues.
-
- World Health Organization. Final Report of the Commission on Social Determinants of Health. Geneva; 2008. Closing the gap in a generation. Health equity through action on the social determinants of health; p. 246. - PubMed
-
- Marmot MG. Strategic review of health inequalities in England post 2010. London: UK Department of Health; 2010. Fair society healthy lives. The Marmot Review; p. 242.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
