

Role of physical training in heart failure with preserved ejection fraction
- PMID: 22430146
- PMCID: PMC4415355
- DOI: 10.1007/s11897-012-0087-7
Role of physical training in heart failure with preserved ejection fraction
Abstract
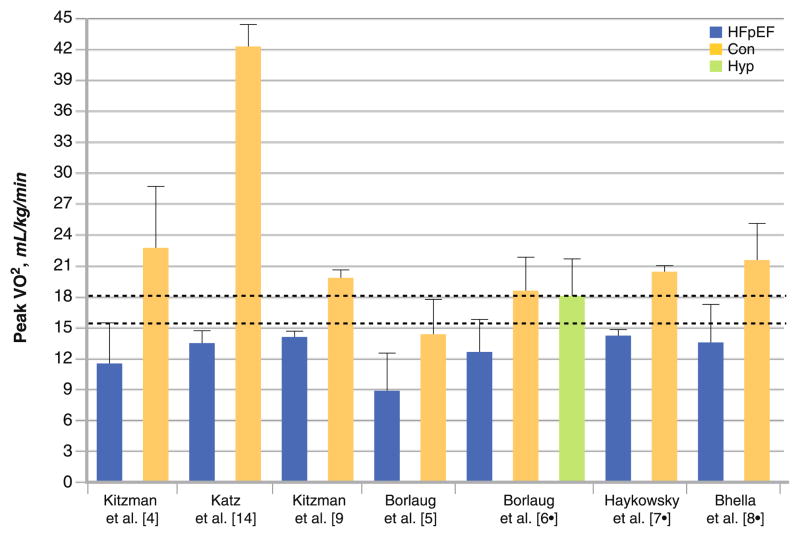
About 50% or more of heart failure (HF) patients living in the community have preserved left ventricular ejection fraction (HFpEF), and the proportion is higher among women and the very elderly. A cardinal feature of HFpEF is reduced aerobic capacity, measured objectively as peak exercise pulmonary oxygen uptake (peak VO(2)), that results in decreased quality of life. Specifically, peak VO(2) of HFpEF patients is 30-70% lower than age-, sex-, and comorbidity-matched control patients without HF. The mechanisms for the reduced peak VO(2) are due to cardiovascular and skeletal muscle dysfunction that results in reduced oxygen delivery to and/or utilization by the active muscles. Currently, four randomized controlled exercise intervention trials have been performed in HFpEF patients. These studies have consistently demonstrated that 3-6 months of aerobic training performed alone or in combination with strength training is a safe and effective therapy to increase aerobic capacity and endurance and quality of life in HFpEF patients. Despite these benefits, the physiologic mechanisms underpinning the improvement in peak exercise performance have not been studied; therefore, future studies are required to determine the role of physical training to reverse the impaired cardiovascular and skeletal muscle function in HFpEF patients.
Figures
References
-
- Kitzman DW, Gardin JM, Gottdiener JS, Arnold A, Boineau R, Aurigemma G, Marino EK, Lyles M, Cushman M, Enright PL. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol. 2001;87(4):413–9. - PubMed
-
- Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol. 1999;33(7):1948–55. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355(3):260–9. - PubMed
-
- Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan MJ. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol. 1991;17(5):1065–72. - PubMed
-
- Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation. 2006;114(20):2138–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
