

Occurrence and impact of intracranial pressure elevation during treatment of severe intraventricular hemorrhage
- PMID: 22430237
- PMCID: PMC4365868
- DOI: 10.1097/CCM.0b013e318241e380
Occurrence and impact of intracranial pressure elevation during treatment of severe intraventricular hemorrhage
Abstract
Objectives: Elevated intracranial pressure is one of the proposed mechanisms leading to poor outcomes in patients with intraventricular hemorrhage. We sought to characterize the occurrence and significance of intracranial hypertension in severe intraventricular hemorrhage requiring extraventricular drainage.
Design: Prospective analysis from two randomized, multicenter, clinical trials.
Setting: Intensive care units of 23 academic hospitals.
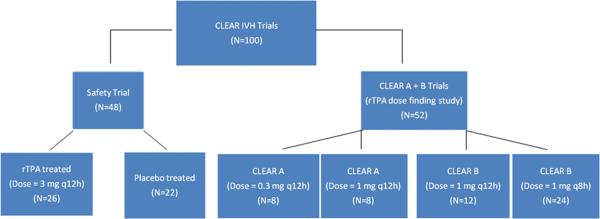
Patients: One hundred patients with obstructive intraventricular hemorrhage and intracerebral hemorrhage volume <30 mL requiring emergency extraventricular drainage from two randomized multicenter studies comparing intraventricular recombinant tissue plasminogen activator (n=78) to placebo (n=22).
Interventions: Intracranial pressure was recorded every 4 hrs in all patients and before and after a 1-hr extraventricular drainage closure period after injection. Intracranial pressure readings were analyzed at predefined thresholds and compared between treatment groups, before and after injection of study agent, and before and after opening of third and fourth ventricles on computed tomography. Impact on 30-day outcomes was assessed.
Measurements and main results: Initial intracranial pressure ranged from -2 to 60 mm Hg (median; interquartile range, 11;10). Of 2576 intracranial pressure readings, 91.5% (2359) were ≤20 mm Hg, 1.6% were >30, 0.5% were >40, and 0.2% were >50 mm Hg. In a multivariate analysis, threshold events>20 mm Hg and >30 mm Hg were more frequent in placebo vs. recombinant tissue plasminogen activator-treated groups (p=.03 and p=.08, respectively). Intracranial pressure elevation>20 mm Hg occurred during a required 1-hr extraventricular drainage closure interval in 207 of 868 (23.8%) injections of study agent, although early reopening of the extraventricular drainage only occurred in 7.9%. After radiographic opening of the lower ventricular system, intracranial pressure events>20 mm Hg remained significantly associated with initial intraventricular hemorrhage volume (p=.002) and extraventricular drainage placement ipsilateral to the largest intraventricular hemorrhage volume (p=.001), but not with thrombolytic treatment (p=.05) or intracerebral hemorrhage volume (p=.14). Ventriculoperitoneal shunts were required in 13.6% of placebo and 6.4% of recombinant tissue plasminogen activator-treated patients (p=.37). Percentage of intracranial pressure readings per patient>30 mm Hg and initial intracerebral hemorrhage and intraventricular hemorrhage volumes were independent predictors of 30-day mortality after adjustment for other outcome predictors (p=.003, p=.03, and p<.001, respectively). Independent predictors of poor modified Rankin Scale score at 30 days were percent of intracranial pressure events>30 mm Hg per patient (p=.01; but not >20 mm Hg), both intracerebral hemorrhage and intraventricular hemorrhage volume, and pulse pressure.
Conclusions: Intracranial pressure is not frequently elevated during monitoring and drainage with an extraventricular drainage in patients with severe intraventricular hemorrhage, although intracranial pressure >30 mm Hg predicts higher short-term mortality. Thrombolytic therapy may reduce the frequency of high intracranial pressure events. Intracranial pressure elevation appears to be significantly correlated with extraventricular drainage placement in the ventricle with greatest clot volume.
Figures


Comment in
-
Novel insights into the pathophysiology and treatment of intraventricular hemorrhage.Crit Care Med. 2012 May;40(5):1683-5. doi: 10.1097/CCM.0b013e3182451e07. Crit Care Med. 2012. PMID: 22511164 No abstract available.
-
Intracranial monitoring and continuous data collection.Crit Care Med. 2012 Nov;40(11):3115-6; author reply 3116. doi: 10.1097/CCM.0b013e31826563c8. Crit Care Med. 2012. PMID: 23080469 No abstract available.
References
-
- de Weerd AW. The prognosis of intraventricular hemorrhage. J Neurol. 1979;222:46–51. - PubMed
-
- Graeb DA, Robertson WD, Lapointe JS, Nugent RA, Harrison PB. Computed tomographic diagnosis of intraventricular hemorrhage. Etiology and prognosis. Radiology. 1982;143:91–6. - PubMed
-
- Todo T, Usui M, Takakura K. Treatment of severe intraventricular hemorrhage by intraventricular infusion of urokinase. J Neurosurg. 1991;74:81–6. - PubMed
-
- Bhattathiri PS, Gregson B, Prasad KS, Mendelow AD. STICH Investigators. Intraventricular hemorrhage and hydrocephalus after spontaneous intracerebral hemorrhage: results from the STICH trial. Acta Neurochir Suppl. 2006;96:65–8. - PubMed
-
- Steiner T, Diringer MN, Schneider D, Mayer SA, Begtrup K, Broderick J, Skolnick BE, Davis SM. Dynamics of intraventricular hemorrhage in patients with spontaneous intracerebral hemorrhage: risk factors, clinical impact, and effect of hemostatic therapy with recombinant activated factor VII. Neurosurgery. 2006 Oct;59(4):767–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
