

An aggressive aneurysmal bone cyst of the proximal humerus and related complications in a pediatric patient
- PMID: 22430999
- PMCID: PMC3332324
- DOI: 10.1007/s11751-012-0132-9
An aggressive aneurysmal bone cyst of the proximal humerus and related complications in a pediatric patient
Abstract
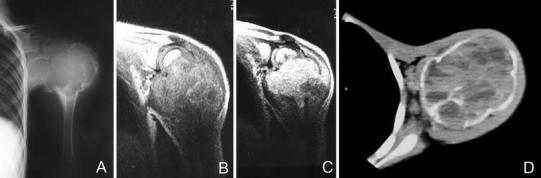
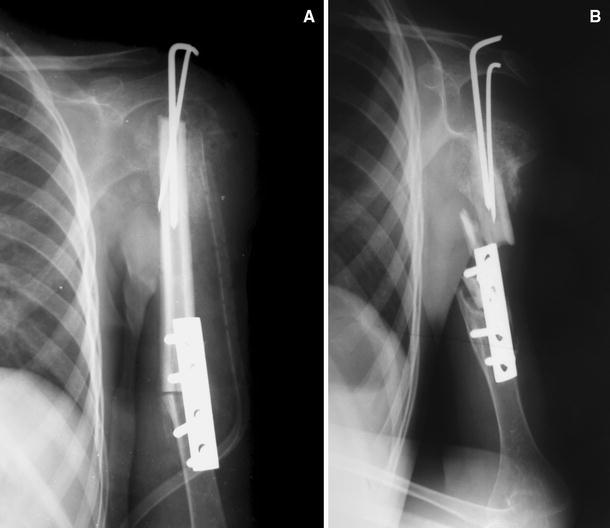
Clinical behavior of aneurysmal bone cyst (ABC) in younger patients can be more aggressive than that in older children and adults. Angular deformity and shortening can occur due to growth plate destruction or tumor resection. A 11-year-old boy who had been operated twice in another center for an ABC located in the left proximal humerus presented to the author's institution with complaints of pain, deformity and shortening of the left arm. Plain radiographs revealed left proximal humerus nonunion with a large defect. Reconstruction with nonvascularized fibular autograft was applied and left upper extremity was immobilized in a velpou bandage. At the third-month follow-up, graft incorporation was observed in the distal part; however, proximal part did not show adequate healing on radiographs. Additional immobilization in a sling for 3 months was advised to the patient and his family. However, they were lost to follow-up and readmitted to the author's institution at the 12th month postoperatively. Radiographs showed failure of the fibular graft fixation and nonunion of the humerus. Autogenic bone grafts, either vascularized or nonvascularized are the best treatment method for the large defects after tumor curettage or resection. Nonvascularized grafts are technically much easier to use than vascularized grafts and provide excellent structural bone support at the recipient side. However, they may take several months to be fully incorporated. In addition, good therapeutic outcomes require patience and collaboration with the patient and parents. Most importantly, the patient should be monitored closely.
Figures



References
-
- Ramirez AR, Stanton RP. Aneurysmal bone cyst in 29 children. J Pediatr Orthop. 2002;22(4):533–539. - PubMed
-
- Gibbs CP, Jr, Hefele MC, Peabody TD, et al. Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am. 1999;81(12):1671–1678. - PubMed
LinkOut - more resources
Full Text Sources
