

Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS)
- PMID: 22431708
- PMCID: PMC3529546
- DOI: 10.1093/ndt/gfs021
Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS)
Abstract
Background: Longer dialysis session length (treatment time, TT) has been associated with better survival among hemodialysis (HD) patients. The impact of TT on clinical markers that may contribute to this survival advantage is not well known.
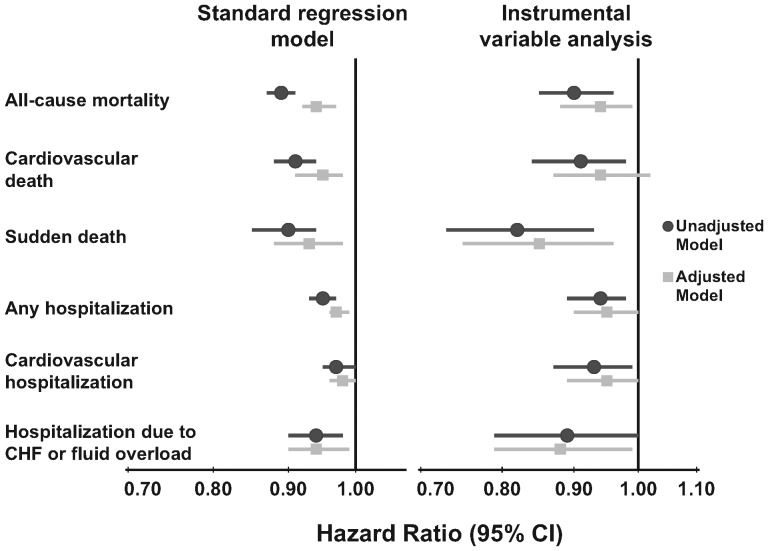
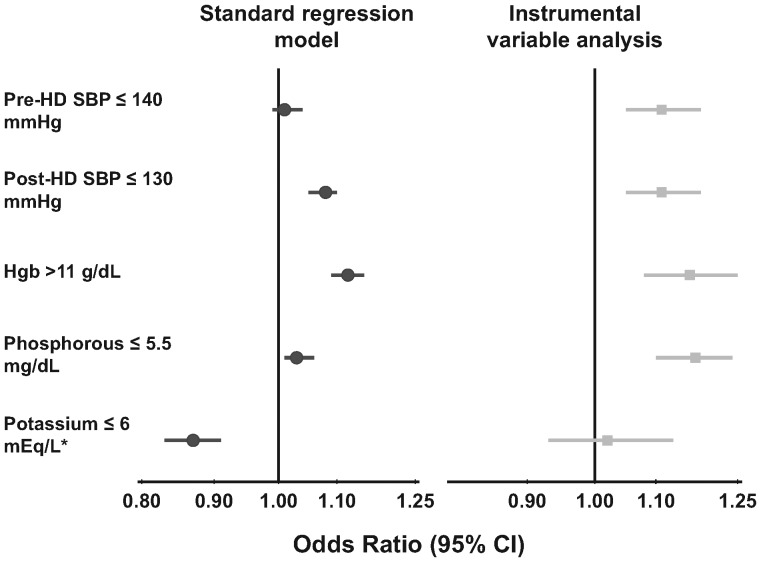
Methods: Using data from the international Dialysis Outcomes and Practice Patterns Study, we assessed the association of TT with clinical outcomes using both standard regression analyses and instrumental variable approaches. The study included 37,414 patients on in-center HD three times per week with prescribed TT from 120 to 420 min.
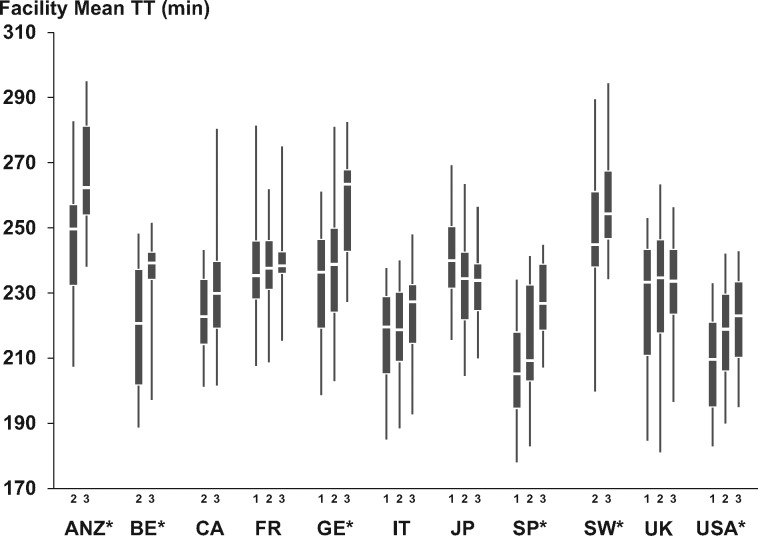
Results: Facility mean TT ranged from 214 min in the USA to 256 min in Australia-New Zealand. Accounting for country effects, mortality risk was lower for patients with longer TT {hazard ratio for every 30 min: all-cause mortality: 0.94 [95% confidence interval (CI): 0.92-0.97], cardiovascular mortality: 0.95 (95% CI: 0.91-0.98) and sudden death: 0.93 (95% CI: 0.88-0.98)}. Patients with longer TT had lower pre- and post-dialysis systolic blood pressure, greater intradialytic weight loss, higher hemoglobin (for the same erythropoietin dose), serum albumin and potassium and lower serum phosphorus and white blood cell counts. Similar associations were found using the instrumental variable approach, although the positive associations of TT with weight loss and potassium were lost.
Conclusions: Favorable levels of a variety of clinical markers may contribute to the better survival of patients receiving longer TT. These findings support longer TT prescription in the setting of in-center, three times per week HD.
Figures
Comment in
-
Dialysis Duration: The longer the better, but why? [corrected].Nephrol Dial Transplant. 2012 Nov;27(11):3975-8. doi: 10.1093/ndt/gfs435. Nephrol Dial Transplant. 2012. PMID: 23144067 No abstract available.
References
-
- US Renal Data System. USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2010.
-
- Suri RS, Nesrallah GE, Mainra R, et al. Daily hemodialysis: a systematic review. Clin J Am Soc Nephrol. 2006;1:33–42. - PubMed
-
- Walsh M, Culleton B, Tonelli M, et al. A systematic review of the effect of nocturnal hemodialysis on blood pressure, left ventricular hypertrophy, anemia, mineral metabolism, and health-related quality of life. Kidney Int. 2005;67:1500–1508. - PubMed
-
- Charra B. Fluid balance, dry weight, and blood pressure in dialysis. Hemodial Int. 2007;11:21–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
