

An autopsy study describing causes of death and comparing clinico-pathological findings among hospitalized patients in Kampala, Uganda
- PMID: 22432042
- PMCID: PMC3303855
- DOI: 10.1371/journal.pone.0033685
An autopsy study describing causes of death and comparing clinico-pathological findings among hospitalized patients in Kampala, Uganda
Abstract
Background: Information on causes of death in HIV-infected patients in Sub-Saharan Africa is mainly derived from observational cohort and verbal autopsy studies. Autopsy is the gold standard to ascertain cause of death. We conducted an autopsy study to describe and compare the clinical and autopsy causes of death and contributory findings in hospitalized HIV-infected and HIV-uninfected patients in Uganda.
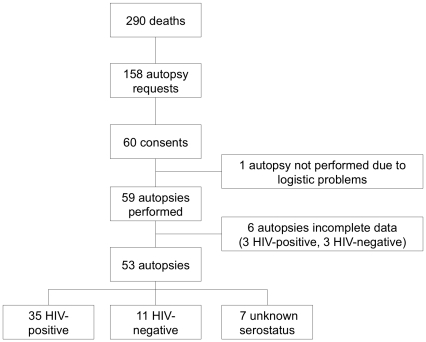
Methods: Between May and September 2009 a complete autopsy was performed on patients that died on a combined infectious diseases gastroenterology ward in Mulago Hospital in Kampala, Uganda. Autopsy cause of death and contributing findings were based on the macro- and microscopic post-mortem findings combined with clinical information. Clinical diagnoses were reported by the ward doctor and classified as confirmed, highly suspected, considered or not considered, based on information derived from the medical chart. Results are reported according to HIV serostatus.
Results: Fifty-three complete autopsies were performed in 66% HIV-positive, 21% HIV-negative and 13% patients with an unknown HIV serological status. Infectious diseases caused death in 83% of HIV-positive patients, with disseminated TB as the main diagnosis causing 37% of deaths. The spectrum of illness and causes of death were substantially different between HIV-positive and HIV-negative patients. In HIV-positive patients 12% of postmortem diagnoses were clinically confirmed, 27% highly suspected, 16% considered and 45% not considered. In HIV-negative patients 17% of postmortem diagnoses were clinically highly suspected, 42% considered and 42% not considered.
Conclusion: Autopsy examination remains an important tool to ascertain causes of death particularly in settings with limited access to diagnostic testing during life. HIV-positive patients continue to die from treatable and clinically undiagnosed infectious diseases. Until rapid-point of care testing is available to confirm common infections, empiric treatment should be further investigated.
Conflict of interest statement
Figures
References
-
- UNAIDS. 2010. Global report: UNAIDS report on the global AIDS epidemic 2010.
-
- Uganda AIDS Commision. 2007. Moving Toward Universal Access: National HIV&AIDS Strategic Plan 2007/8–2011/12.
-
- Beadsworth MB, Cohen D, Ratcliffe L, Jenkins N, Taylor W, et al. Autopsies in HIV: still identifying missed diagnoses. Int J STD AIDS. 2009;20:84–86. - PubMed
-
- Shojania KG, Burton EC, McDonald KM, Goldman L. Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA. 2003;289:2849–2856. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
