

Hormone replacement therapy and physical function in healthy older men. Time to talk hormones?
- PMID: 22433122
- PMCID: PMC5393154
- DOI: 10.1210/er.2012-1002
Hormone replacement therapy and physical function in healthy older men. Time to talk hormones?
Abstract
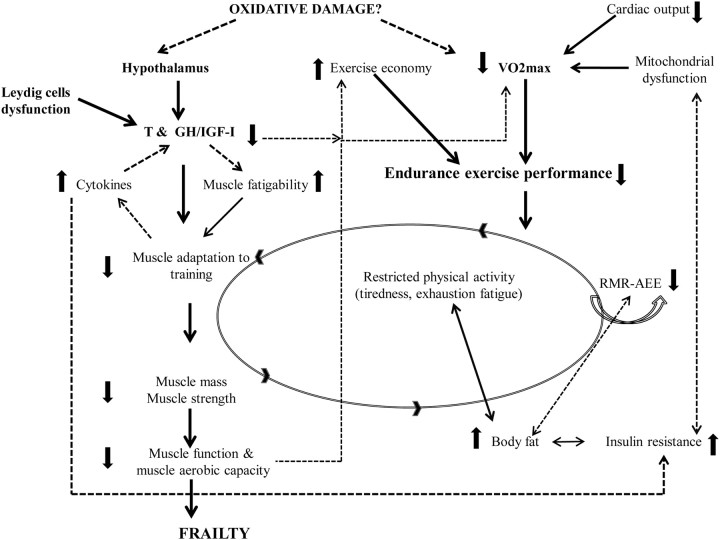
Improving physical function and mobility in a continuously expanding elderly population emerges as a high priority of medicine today. Muscle mass, strength/power, and maximal exercise capacity are major determinants of physical function, and all decline with aging. This contributes to the incidence of frailty and disability observed in older men. Furthermore, it facilitates the accumulation of body fat and development of insulin resistance. Muscle adaptation to exercise is strongly influenced by anabolic endocrine hormones and local load-sensitive autocrine/paracrine growth factors. GH, IGF-I, and testosterone (T) are directly involved in muscle adaptation to exercise because they promote muscle protein synthesis, whereas T and locally expressed IGF-I have been reported to activate muscle stem cells. Although exercise programs improve physical function, in the long-term most older men fail to comply. The GH/IGF-I axis and T levels decline markedly with aging, whereas accumulating evidence supports their indispensable role in maintaining physical function integrity. Several studies have reported that the administration of T improves lean body mass and maximal voluntary strength in healthy older men. On the other hand, most studies have shown that administration of GH alone failed to improve muscle strength despite amelioration of the detrimental somatic changes of aging. Both GH and T are anabolic agents that promote muscle protein synthesis and hypertrophy but work through separate mechanisms, and the combined administration of GH and T, albeit in only a few studies, has resulted in greater efficacy than either hormone alone. Although it is clear that this combined approach is effective, this review concludes that further studies are needed to assess the long-term efficacy and safety of combined hormone replacement therapy in older men before the medical rationale of prescribing hormone replacement therapy for combating the sarcopenia of aging can be established.
Figures
Similar articles
-
Single and combined effects of growth hormone and testosterone administration on measures of body composition, physical performance, mood, sexual function, bone turnover, and muscle gene expression in healthy older men.J Clin Endocrinol Metab. 2002 Dec;87(12):5649-57. doi: 10.1210/jc.2002-020098. J Clin Endocrinol Metab. 2002. PMID: 12466367 Clinical Trial.
-
Loss of lean body and muscle mass correlates with androgen levels in hypogonadal men with acquired immunodeficiency syndrome and wasting.J Clin Endocrinol Metab. 1996 Nov;81(11):4051-8. doi: 10.1210/jcem.81.11.8923860. J Clin Endocrinol Metab. 1996. PMID: 8923860
-
Testosterone and growth hormone improve body composition and muscle performance in older men.J Clin Endocrinol Metab. 2009 Jun;94(6):1991-2001. doi: 10.1210/jc.2008-2338. Epub 2009 Mar 17. J Clin Endocrinol Metab. 2009. PMID: 19293261 Free PMC article. Clinical Trial.
-
Androgen replacement therapy to reverse and/or prevent age-associated sarcopenia in men.Baillieres Clin Endocrinol Metab. 1998 Oct;12(3):419-25. doi: 10.1016/s0950-351x(98)80153-5. Baillieres Clin Endocrinol Metab. 1998. PMID: 10332563 Review.
-
Anabolic processes in human skeletal muscle: restoring the identities of growth hormone and testosterone.Phys Sportsmed. 2010 Oct;38(3):97-104. doi: 10.3810/psm.2010.10.1814. Phys Sportsmed. 2010. PMID: 20959702 Review.
Cited by
-
Late-onset hypogonadism: current concepts and controversies of pathogenesis, diagnosis and treatment.Asian J Androl. 2014 Mar-Apr;16(2):192-202. doi: 10.4103/1008-682X.122336. Asian J Androl. 2014. PMID: 24407185 Free PMC article. Review.
-
Sarcopenia: A Contemporary Health Problem among Older Adult Populations.Nutrients. 2020 May 1;12(5):1293. doi: 10.3390/nu12051293. Nutrients. 2020. PMID: 32370051 Free PMC article. Review.
-
Effect of weight loss, exercise, or both on cognition and quality of life in obese older adults.Am J Clin Nutr. 2014 Jul;100(1):189-98. doi: 10.3945/ajcn.113.082883. Epub 2014 Apr 30. Am J Clin Nutr. 2014. PMID: 24787497 Free PMC article. Clinical Trial.
-
Prevalence of Sarcopenic Obesity in Various Comorbidities, Diagnostic Markers, and Therapeutic Approaches: A Review.Ann Geriatr Med Res. 2022 Dec;26(4):296-308. doi: 10.4235/agmr.22.0081. Epub 2022 Nov 18. Ann Geriatr Med Res. 2022. PMID: 36397294 Free PMC article.
-
Metabolic Effects of Testosterone Hormone Therapy in Normal and Orchiectomized Male Rats: From Indirect Calorimetry to Lipolytic Enzymes.Int J Endocrinol. 2019 Nov 28;2019:7546385. doi: 10.1155/2019/7546385. eCollection 2019. Int J Endocrinol. 2019. PMID: 31871453 Free PMC article.
References
-
- 2007. Administration on Aging. Federal Interagency Forum on Aging-Related Statistics. [electronic mail system]. http://www.aoa.gov/AoAroot/Aging_Statistics/Profile/2007/4.aspx
-
- Adams PF , Dey AN , Vickerie JL. 2007. Summary health statistics for the U.S. population: National Health Interview Survey, 2005. Vital Health Stat 10 233:1–104 - PubMed
-
- Nagi SZ. 1965. Rehab in the engineering classroom. Rehabil Rec 6:20–21 - PubMed
-
- Applegate WB , Blass JP , Williams TF. 1990. Instruments for the functional assessment of older patients. N Engl J Med 322:1207–1214 - PubMed
-
- Fried LP , Tangen CM , Walston J , Newman AB , Hirsch C , Gottdiener J , Seeman T , Tracy R , Kop WJ , Burke G , McBurnie MA. 2001. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M146–M156 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
