

Patterns of regional lymph node metastasis of nasopharyngeal carcinoma: a meta-analysis of clinical evidence
- PMID: 22433671
- PMCID: PMC3353248
- DOI: 10.1186/1471-2407-12-98
Patterns of regional lymph node metastasis of nasopharyngeal carcinoma: a meta-analysis of clinical evidence
Abstract
Background: The characteristics of cervical lymphatic metastasis in nasopharyngeal carcinoma (NPC) are not completely understood. As such, radiotherapy to the entire lymphatic of the neck bilaterally has been empirically practiced even in early stage disease, although not supported by clinical evidence. We studied the pattern and probability of nodal metastasis through a meta-analysis of published evidences, with an aim to establish an evidence-based guideline for selecting and delineation of clinical target volume of neck lymphatics for conformation radiation for NPC.
Methods: A literature search yielded an initial 411 original articles, and 13 studies with 2920 NPC cases staged via MRI were included in this analysis. The occurrence of nodal metastasis was calculated and analyzed according to the respective regional nodal levels.
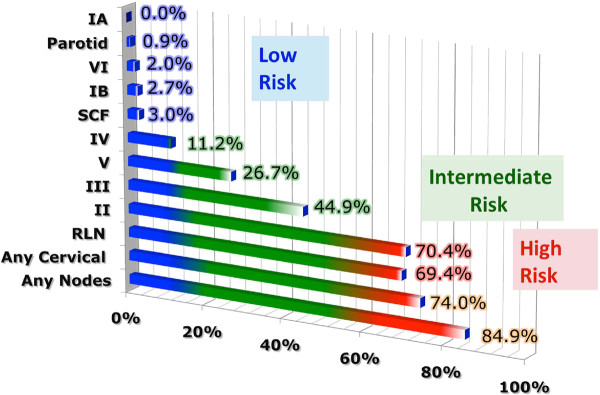
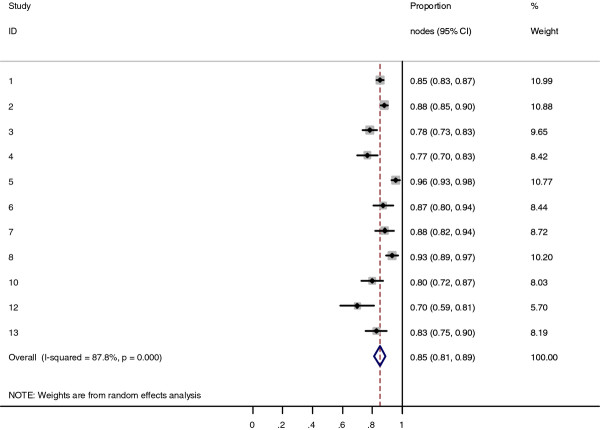
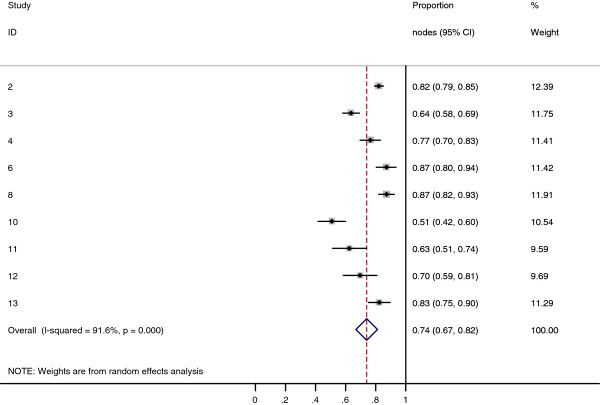
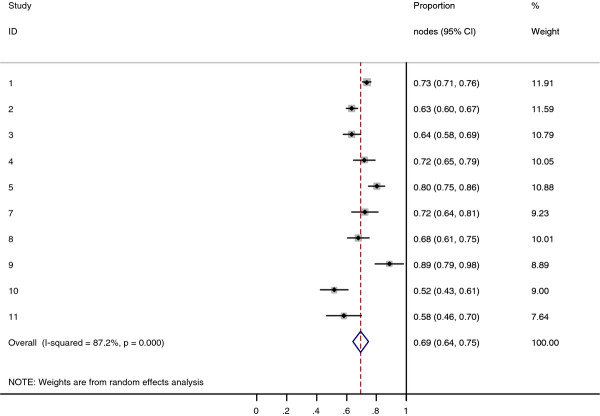
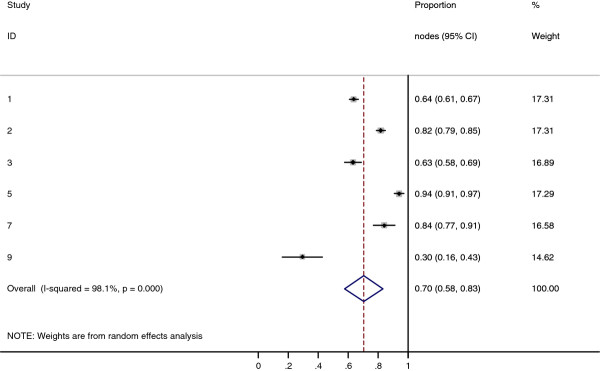
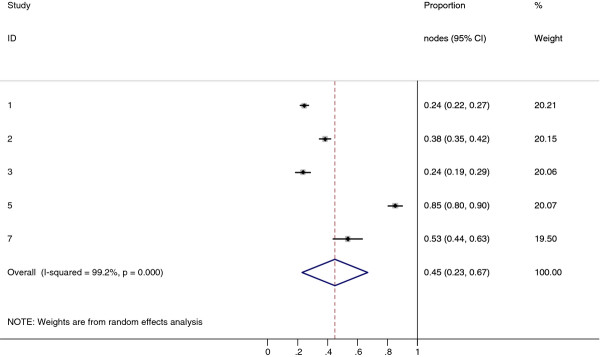
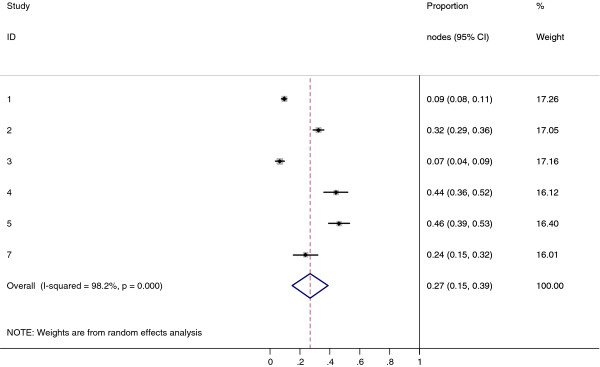
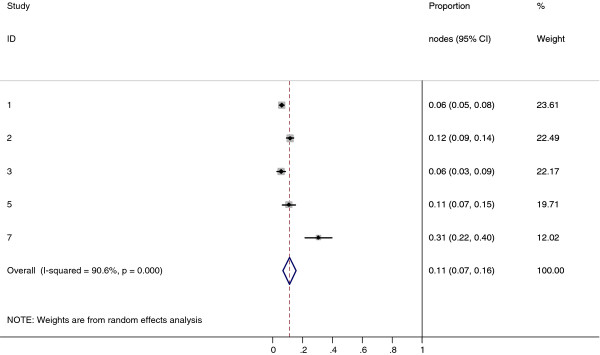
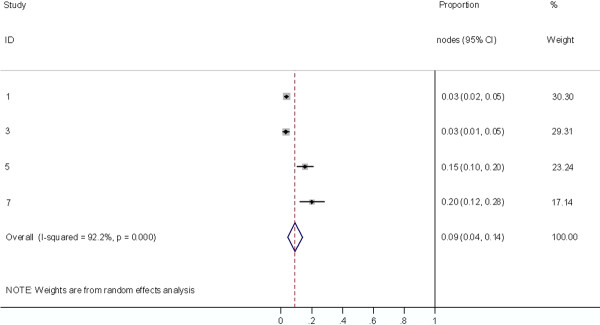
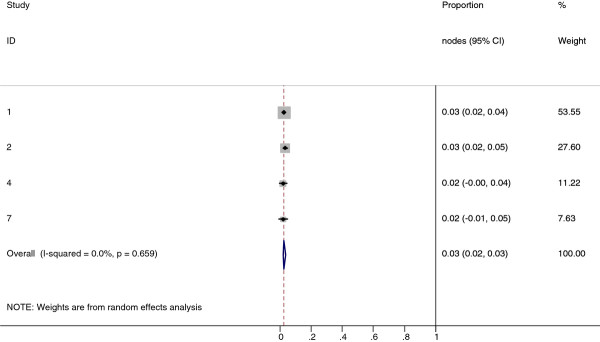
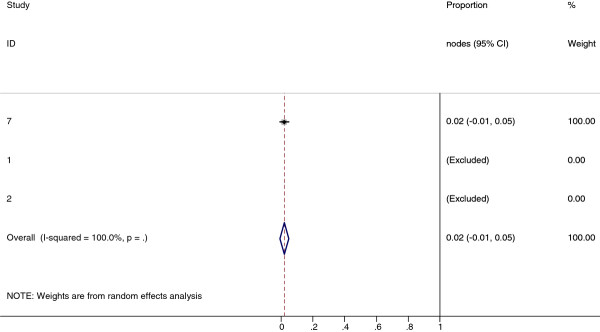
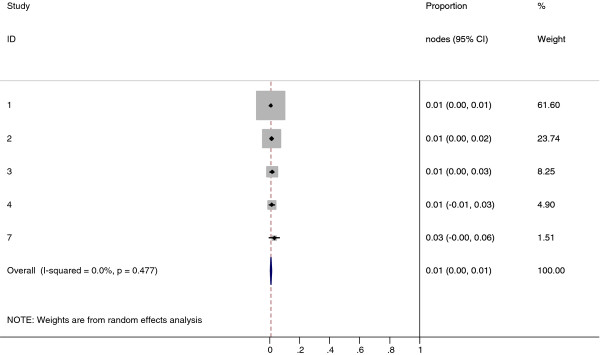
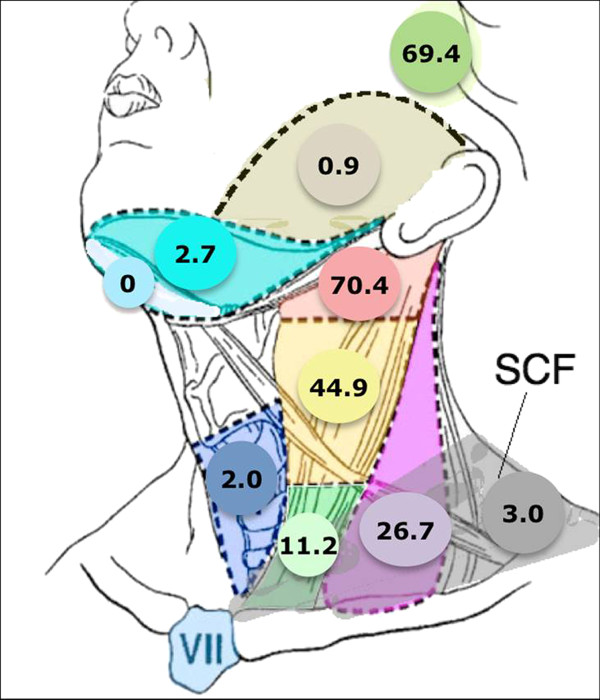
Results: 85% of NPC cases presented with lymphadenopathy. The most commonly involved regions include retropharyngeal (69%) and level II lymph nodes (70%). The overall probability of levels III, IV, and V nodal involvement are 45%, 11%, and 27%, respectively. Low-risk node groups included the supraclavicular, levels IA/IB and VI nodes, and parotid nodes with involvement rates at 3%, 0%, 3%, 0%, and 1%, respectively. Nodal metastases followed an orderly pattern and the probability of "skip" metastasis between levels varied between 0.5-7.9%.
Conclusions: Lymph node metastasis in NPC follows a predictable and orderly pattern. The rarity of metastasis in certain nodal groups and "skip" metastasis suggest that reduced treatment volume is feasible in conformal radiotherapy for NPC.
Figures

References
-
- Parkin WS DM, Ferlay RL J, Young J. Cancer Incidence in Five Continents, Vol 7. Vol. 7. Lyon: IARC Press; 1997.
-
- CA P. Principles and Practice of Radiation Oncolog. 3. Philadelphia: JB Lippincott; 1998. Nasopharynx.
-
- Lee AW, Ng WT, Hung WM, Choi CW, Tung R, Ling YH, Cheng PT, Yau TK, Chang AT, Leung SK. et al. Major late toxicities after conformal radiotherapy for nasopharyngeal carcinoma-patient- and treatment-related risk factors. Int J Radiat Oncol Biol Phys. 2009;73(4):1121–1128. doi: 10.1016/j.ijrobp.2008.05.023. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
