

Imaging biomarkers of brain tumour margin and tumour invasion
- PMID: 22433826
- PMCID: PMC3473903
- DOI: 10.1259/bjr/26838774
Imaging biomarkers of brain tumour margin and tumour invasion
Abstract
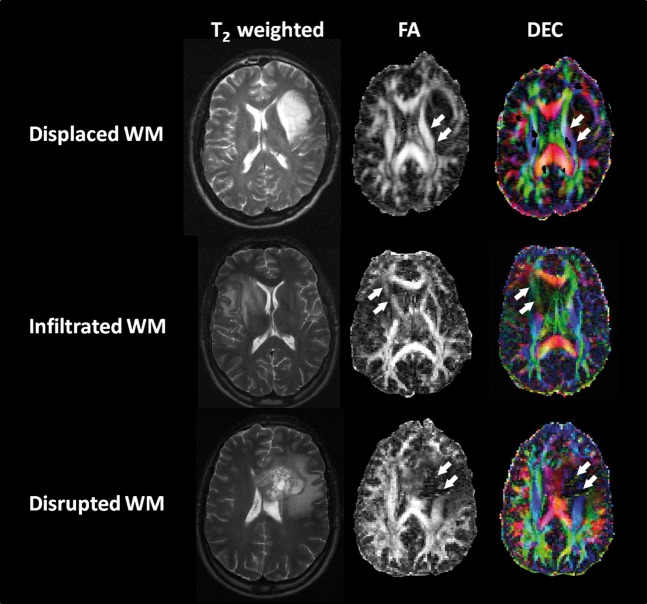
Invasion of tumour cells into the normal brain is one of the major reasons of treatment failure for gliomas. Although there is a good understanding of the molecular and cellular processes that occur during this invasion, it is not possible to detect the extent of the tumour with conventional imaging. However, there is an understanding that the degree of invasion differs with individual tumours, and yet they are all treated the same. Newer imaging techniques that probe the pathological changes within tumours may be suitable biomarkers for invasion. Imaging methods are now available that can detect subtle changes in white matter organisation (diffusion tensor imaging), tumour metabolism and cellular proliferation (using MR spectroscopy and positron emission tomography) occurring in regions of tumour that cannot be detected by conventional imaging. The role of such biomarkers of invasion should allow better delineation of tumour margins, which should improve treatment planning (especially surgery and radiotherapy) and provide information on the invasiveness of an individual tumour to help select the most appropriate therapy and help stratify patients for clinical trials.
Figures



References
-
- Stupp R, Mason WP, van denBent MJ, Weller M, Fisher B, Taphoorn MJB, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–96 - PubMed
-
- Dandy WE. Removal of the right hemisphere for certain tumors with hemiplegia: preliminary report. J Am Med Assoc 1928;90:823–5
-
- Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21:109–22 - PubMed
-
- Lee SW, Fraass BA, Marsh LH, Herbort K, Gebarski SS, Martel MK, et al. Patterns of failure following high-dose 3-D conformal radiotherapy for high-grade astrocytomas: a quantitative dosimetric study. Int J Radiat Oncol Biol Phys 1999;43:79–88 - PubMed
-
- Oppitz U, Maessen D, Zunterer H, Richter S, Flentje M. 3D-recurrence-patterns of glioblastomas after CT-planned postoperative irradiation. Radiother Oncol 1999;53:53–7 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
