

Anticipatory planning of functional reach-to-grasp: a pilot study
- PMID: 22434022
- PMCID: PMC6015502
- DOI: 10.1177/1545968312437938
Anticipatory planning of functional reach-to-grasp: a pilot study
Abstract
Background: Intensive task-oriented training such as constraint-induced movement therapy (CIMT) is thought to engage motor learning and decision-making processes, including anticipatory action planning.
Objective: To identify the effects of CIMT on anticipatory hand posture selection and movement time for task-specific reach-to-grasp performance.
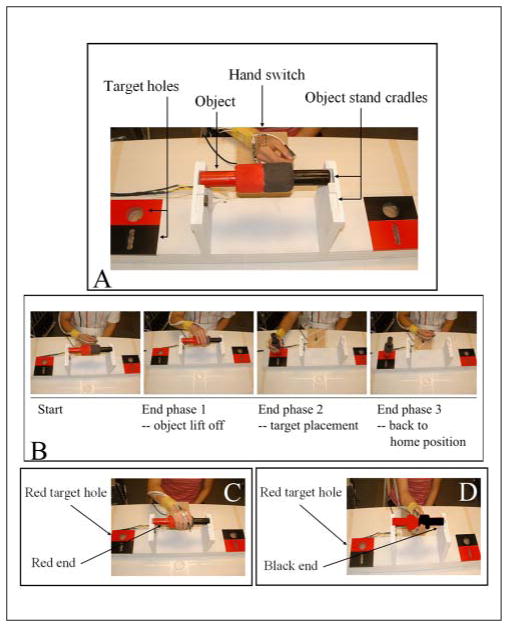
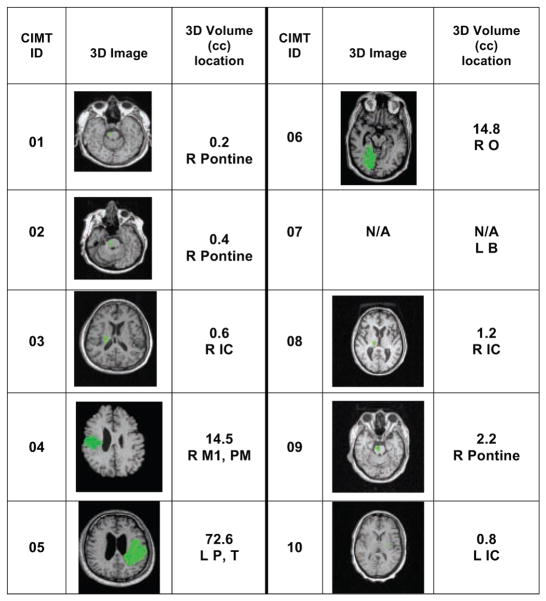
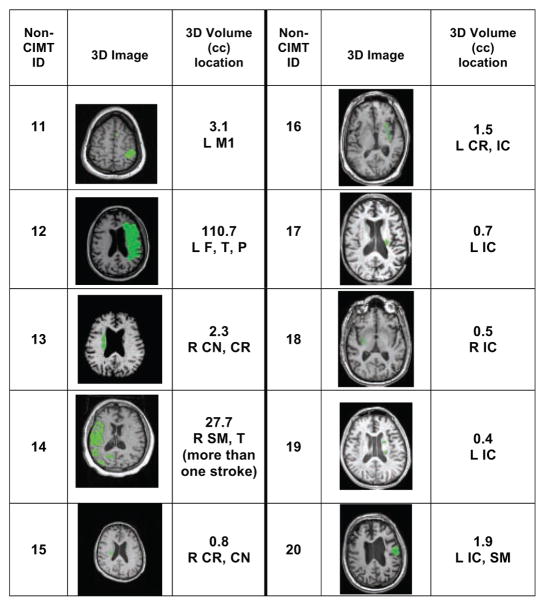
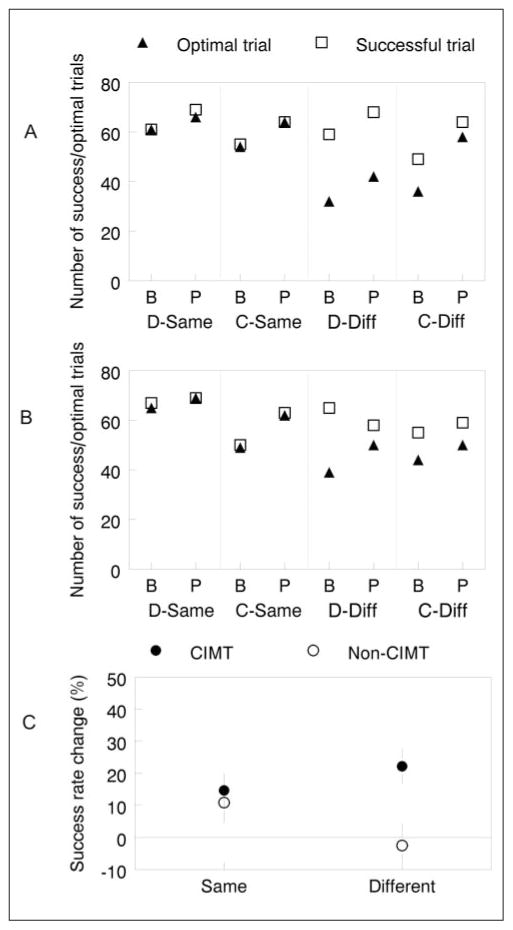
Methods: Subacute and chronic poststroke participants were recruited into CIMT (n = 10) or non-CIMT (n = 10) groups. Arm and hand functions were assessed before and after 2 weeks with the Wolf Motor Function Test (WMFT), Motor Activity Log (MAL), and a unique skilled reach-to-grasp task designed to test anticipatory hand posture selection. The reach-to-grasp tasks included power and precision grasping in 2 conditions achieved optimally with either a pronated (low difficulty) or supinated (high difficulty) hand posture. Outcome measures included success rate, frequency of optimal strategy selection, and movement time.
Results: Between-group comparisons revealed a significant treatment effect for WMFT and MAL scores. The CIMT group showed larger gains in success rate, optimal posture selection (precision grasp only), and faster movement times for the supinated conditions.
Conclusion: Together, a faster movement time and greater frequency of optimal hand posture selection in the more difficult task condition highlights a set of novel findings. These results provide evidence for training-induced improvements in upper-extremity function that support neurobehavioral recovery more than compensation. Although these findings are preliminary in view of the small sample size, the authors suggest that they may be useful to design and power larger-scale studies to further the understanding of the fundamental mechanisms induced by task-oriented training interventions in neurorehabilitation.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Page SJ, Sisto S, Levine P, McGrath RE. Efficacy of modified constraint-induced movement therapy in chronic stroke: a single-blinded randomized controlled trial. Arch Phys Med Rehabil. 2004;85:14–18. - PubMed
-
- Wu C-Y, Chuang L-L, Lin K-C, Chen H-C, Tsay P-K. Randomized trial of distributed CIMT versus bilateral arm training for the rehabilitation of upper-limb motor control and function after stroke. Neurorehabil Neural Repair. 2011;25:130–139. - PubMed
-
- Page SJ, Levine P, Leonard AC. Modified constraint-induced therapy in acute stroke: a randomized controlled pilot study. Neurorehabil Neural Repair. 2005;19:27–32. - PubMed
-
- van der Lee JH, Wagenaar RC, Lankhorst GJ, Vogelaar TW, Deville WL, Bouter LM. Forced use of the upper extremity in chronic stroke patients: results from a single-blind randomized clinical trial. Stroke. 1999;30:2369–2375. - PubMed
-
- Dromerick AW, Edwards DF, Hahn M. Does the application of constraint-induced movement therapy during acute rehabilitation reduce arm impairment after ischemic stroke? Stroke. 2000;31:2984–2988. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
