

Defective tumor necrosis factor release from Crohn's disease macrophages in response to Toll-like receptor activation: relationship to phenotype and genome-wide association susceptibility loci
- PMID: 22434667
- PMCID: PMC3532612
- DOI: 10.1002/ibd.22952
Defective tumor necrosis factor release from Crohn's disease macrophages in response to Toll-like receptor activation: relationship to phenotype and genome-wide association susceptibility loci
Abstract
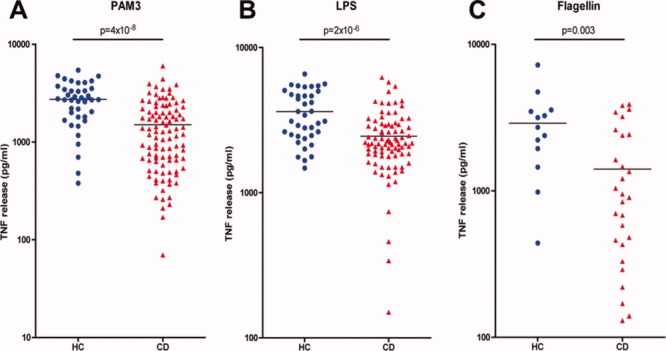
Background: Recent work provides evidence of a failure of acute inflammation in Crohn's disease (CD), and suggests that the primary defect operates at the level of the macrophage and cytokine release. Here we extend the characterization of the innate immune defect in CD by investigating the macrophage response to Toll-like receptor (TLR) agonists and assess potential links between genome-wide association study (GWAS) susceptibility loci, disease phenotype, and therapeutic regimens on tumor necrosis factor α (TNF) release.
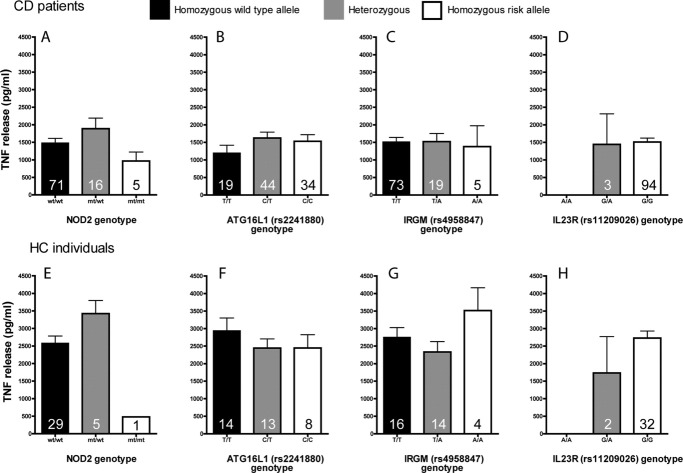
Methods: Peripheral blood-derived macrophages were cultured from control subjects and patients with CD, stimulated with TLR ligands, and the release of TNF measured. Genomic DNA was purified from blood and genotyped for 34 single nucleotide polymorphisms (SNPs) identified as being associated with CD by GWAS.
Results: All stimuli resulted in a reduction (32%-48%) in TNF release from macrophages derived from CD patients (n = 28-101) compared to those from healthy control (HC) subjects. All phenotypes demonstrated impaired TNF release, with the greatest defect in patients with colonic disease. There was no detectable relationship between the level of TNF released and the presence of GWAS susceptibility loci in CD patients. Reduced TNF levels were not influenced by age, gender, or use of aminosalicylate (5-ASA) medication.
Conclusions: This study supports the hypothesis of defective proinflammatory cytokine secretion and an innate immunodeficiency in CD. Abnormal TNF secretion is evident downstream of multiple TLRs, affects all disease phenotypes, and is unrelated to 34 polymorphisms associated with CD by GWAS.
Copyright © 2012 Crohn's & Colitis Foundation of America, Inc.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical