

The efficacy and safety of febuxostat for urate lowering in gout patients ≥65 years of age
- PMID: 22436129
- PMCID: PMC3368715
- DOI: 10.1186/1471-2318-12-11
The efficacy and safety of febuxostat for urate lowering in gout patients ≥65 years of age
Abstract
Background: The incidence of gout rises with increasing age. Management of elderly (≥65 years) gout patients can be challenging due to high rates of comorbidities, such as renal impairment and cardiovascular disease, and concomitant medication use. However, there is little data specifically addressing the efficacy and safety of available urate-lowering therapies (ULT) in the elderly. The objective of this post hoc analysis was to examine the efficacy and safety of ULT with febuxostat or allopurinol in a subset of elderly subjects enrolled in the CONFIRMS trial.
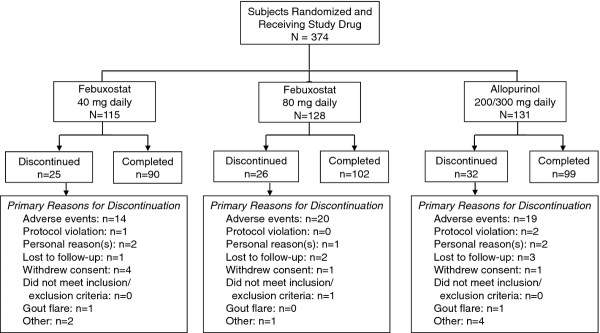
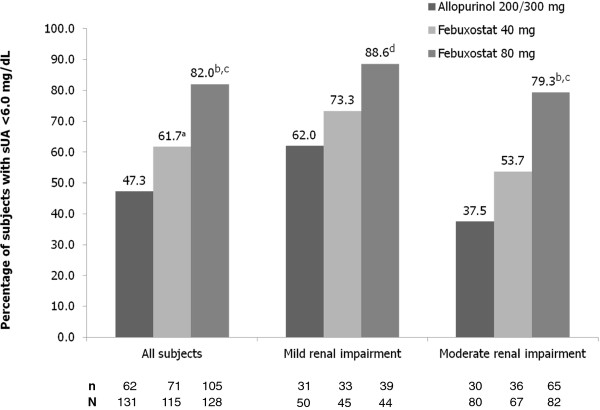
Methods: Hyperuricemic (serum urate [sUA] levels ≥ 8.0 mg/dL) gout subjects were enrolled in the 6-month, double-blind, randomized, comparative CONFIRMS trial and randomized, 1:1:1, to receive febuxostat, 40 mg or 80 mg, or allopurinol (200 mg or 300 mg based on renal function) once daily. Flare prophylaxis was provided throughout the study duration.Study endpoints were the percent of elderly subjects with sUA <6.0 mg/dL at the final visit, overall and by renal function status, percent change in sUA from baseline to final visit, flare rates, and rates of adverse events (AEs).
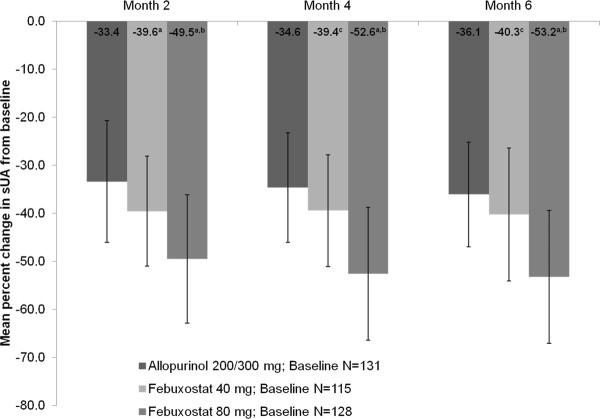
Results: Of 2,269 subjects enrolled, 374 were elderly. Febuxostat 80 mg was significantly more efficacious (82.0%) than febuxostat 40 mg (61.7%; p < 0.001) or allopurinol (47.3%; p < 0.001) for achieving the primary efficacy endpoint. Febuxostat 40 mg was also superior to allopurinol in this population (p = 0.029). In subjects with mild-to-moderate renal impairment, significantly greater ULT efficacy was observed with febuxostat 40 mg (61.6%; p = 0.028) and febuxostat 80 mg (82.5%; p < 0.001) compared to allopurinol 200/300 mg (46.9%). Compared to allopurinol 200/300 mg, the mean percent change in sUA from baseline was significantly greater for both febuxostat 80 mg (p < 0.001) and febuxostat 40 mg (p = 0.011) groups. Flare rates declined steadily in all treatment groups. Rates of AEs were low and comparable across treatments.
Conclusions: These data suggest that either dose of febuxostat is superior to commonly prescribed fixed doses of allopurinol (200/300 mg) in subjects ≥65 years of age with high rates of renal dysfunction. In addition, in this high-risk population, ULT with either drug was well tolerated.
Trial registration: clinicaltrials.gov NCT#00430248.
Trial registration: ClinicalTrials.gov NCT00430248.
Figures
References
-
- Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498–501. - PubMed
-
- National Center for Health Statistics. Health, United States, 2009: With special feature on medical technology. Hyattsville: Centers for Disease Control. U.S. Department of Health and Human Services; 2010. - PubMed
-
- Hande KR, Noone RM, Stone WJ. Severe allopurinol toxicity. Description and guidelines for prevention in patients with renal insufficiency. Am J Med. 1984;76:47–56. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
