

Impact of heterogeneity-based dose calculation using a deterministic grid-based Boltzmann equation solver for intracavitary brachytherapy
- PMID: 22436788
- PMCID: PMC3955059
- DOI: 10.1016/j.ijrobp.2011.12.074
Impact of heterogeneity-based dose calculation using a deterministic grid-based Boltzmann equation solver for intracavitary brachytherapy
Abstract
Purpose: To investigate the dosimetric impact of the heterogeneity dose calculation Acuros (Transpire Inc., Gig Harbor, WA), a grid-based Boltzmann equation solver (GBBS), for brachytherapy in a cohort of cervical cancer patients.
Methods and materials: The impact of heterogeneities was retrospectively assessed in treatment plans for 26 patients who had previously received (192)Ir intracavitary brachytherapy for cervical cancer with computed tomography (CT)/magnetic resonance-compatible tandems and unshielded colpostats. The GBBS models sources, patient boundaries, applicators, and tissue heterogeneities. Multiple GBBS calculations were performed with and without solid model applicator, with and without overriding the patient contour to 1 g/cm(3) muscle, and with and without overriding contrast materials to muscle or 2.25 g/cm(3) bone. Impact of source and boundary modeling, applicator, tissue heterogeneities, and sensitivity of CT-to-material mapping of contrast were derived from the multiple calculations. American Association of Physicists in Medicine Task Group 43 (TG-43) guidelines and the GBBS were compared for the following clinical dosimetric parameters: Manchester points A and B, International Commission on Radiation Units and Measurements (ICRU) report 38 rectal and bladder points, three and nine o'clock, and (D2cm3) to the bladder, rectum, and sigmoid.
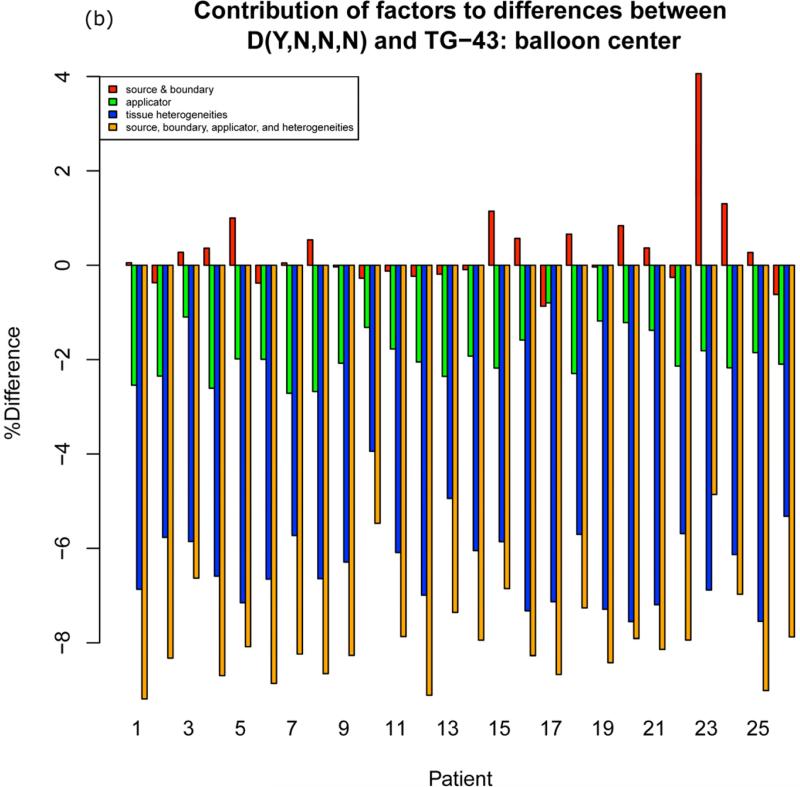
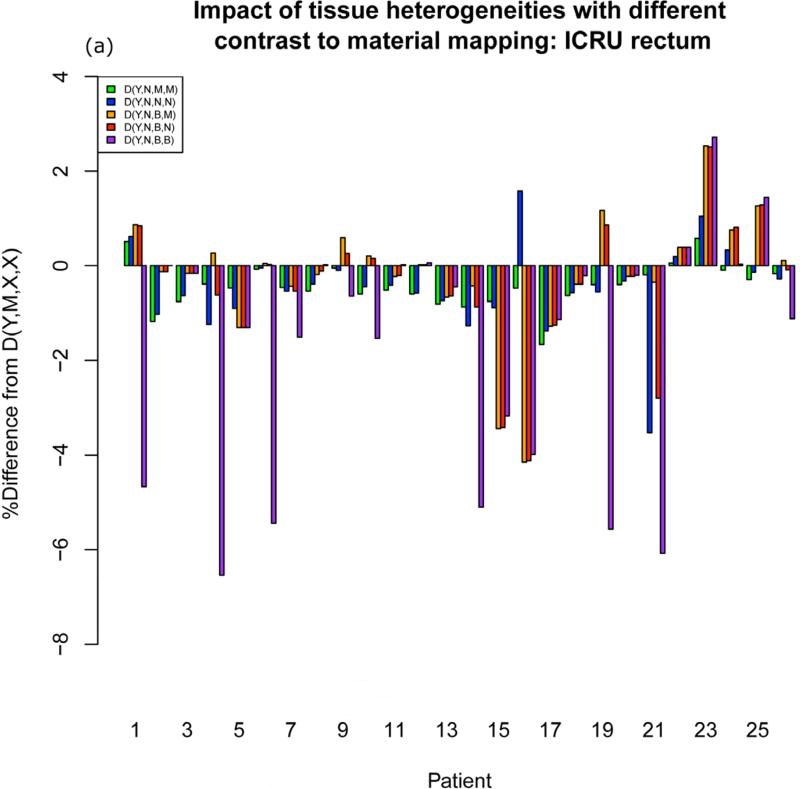
Results: Points A and B, D(2) cm(3) bladder, ICRU bladder, and three and nine o'clock were within 5% of TG-43 for all GBBS calculations. The source and boundary and applicator account for most of the differences between the GBBS and TG-43 guidelines. The D(2cm3) rectum (n = 3), D(2cm3) sigmoid (n = 1), and ICRU rectum (n = 6) had differences of >5% from TG-43 for the worst case incorrect mapping of contrast to bone. Clinical dosimetric parameters were within 5% of TG-43 when rectal and balloon contrast were mapped to bone and radiopaque packing was not overridden.
Conclusions: The GBBS has minimal impact on clinical parameters for this cohort of patients with unshielded applicators. The incorrect mapping of rectal and balloon contrast does not have a significant impact on clinical parameters. Rectal parameters may be sensitive to the mapping of radiopaque packing.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures



References
-
- Viswanathan AN, Erickson BA. Three-dimensional imaging in gynecologic brachytherapy: a survey of the American Brachytherapy Society. Int J Radiat Oncol Biol Phys. 2010;76:104–109. - PubMed
-
- Rivard MJ, Coursey BM, DeWerd LA, et al. Update of AAPM Task Group No. 43 Report: A revised AAPM protocol for brachytherapy dose calculations. Med Phys. 2004;31:633–674. - PubMed
-
- Poon E, Williamson JF, Vuong T, et al. Patient-Specific Monte Carlo Dose Calculations for High-Dose-Rate Endorectal Brachytherapy With Shielded Intracavitary Applicator. Int J Radiat Oncol Biol Phys. 2008;72:1259–1266. - PubMed
-
- Richardson S, Palaniswaamy G, Grigsby PW. Dosimetric effects of air pockets around high-dose rate brachytherapy vaginal cylinders. Int J Radiat Oncol Biol Phys. 2010;78:276–279. - PubMed
-
- Kwan IS, Wilkinson D, Cutajar D, et al. The effect of rectal heterogeneity on wall dose in high dose rate brachytherapy. Med Phys. 2009;36:224–232. - PubMed
