

Relative risk of renal disease among people living with HIV: a systematic review and meta-analysis
- PMID: 22439731
- PMCID: PMC3402981
- DOI: 10.1186/1471-2458-12-234
Relative risk of renal disease among people living with HIV: a systematic review and meta-analysis
Abstract
Background: Antiretroviral therapy (ART) has substantially decreased mortality and HIV-related morbidity. However, other morbidities appear to be more common among PLHIV than in the general population. This study aimed to estimate the relative risk of renal disease among people living with HIV (PLHIV) compared to the HIV-uninfected population.
Methods: We conducted a systematic review and meta-analysis of relative risks of renal disease among populations of PLHIV reported in studies from the peer-reviewed literature. We searched Medline for relevant journal articles published before September 2010, yielding papers published during or after 2002. We also searched conference proceedings of the International AIDS Society (IAS) and Conference on Retroviruses and Opportunistic Infections (CROI) prior to and including 2010. Eligible studies were observational studies reporting renal disease defined as acute or chronic reduced renal function with glomerular filtration rate less than or equal to 60 ml/min/1.73 m2 among HIV-positive adults. Pooled relative risks were calculated for various groupings, including class of ART drugs administered.
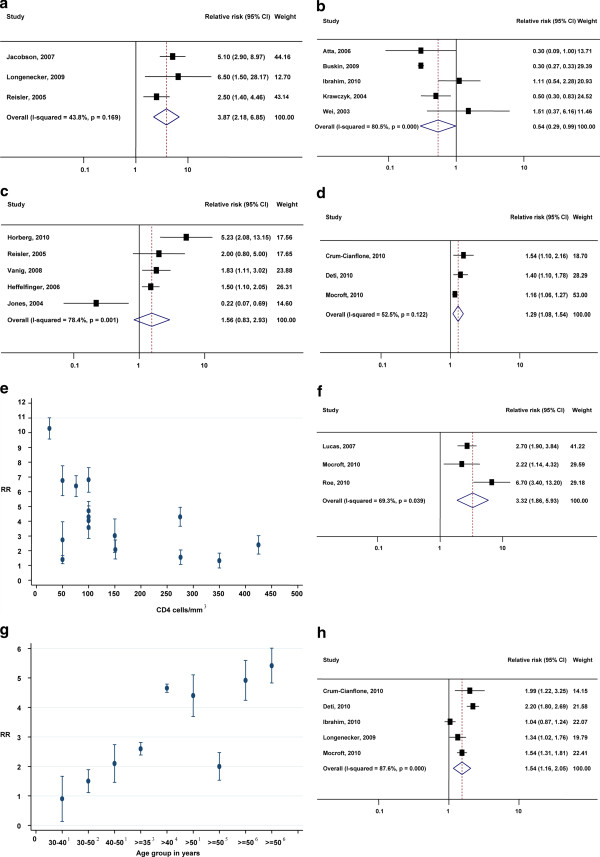
Results: The overall relative risk of renal disease was 3.87 (95% CI: 2.85-6.85) among HIV-infected people compared to HIV-uninfected people. The relative risk of renal disease among people with late-stage HIV infection (AIDS) was 3.32 (1.86-5.93) compared to other PLHIV. The relative risk of renal disease among PLHIV who were receiving antiretroviral therapy (ART) was 0.54 (0.29-0.99) compared to treatment-naïve PLHIV; the relative risk of renal disease among PLHIV who were treated with tenofovir was 1.56 (0.83-2.93) compared to PLHIV who were treated with non-tenofovir therapy. The risk of renal disease was also found to significantly increase with age.
Conclusion: PLHIV are at increased risk of renal disease, with greater risk at later stages of infection and at older ages. ART prolongs survival and decreases the risk of renal disease. However, less reduction in renal disease risk occurs for Tenofovir-containing ART than for other regimens.
Figures

References
-
- Meguid El Nahas A, Bello AK. Chronic kidney disease: the global challenge. Lancet. 2005;365(9456):331–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
