

Endovascular mechanical thrombectomy for the treatment of acute ischemic stroke due to arterial dissection
- PMID: 22440604
- PMCID: PMC3312093
- DOI: 10.1177/159101991201800110
Endovascular mechanical thrombectomy for the treatment of acute ischemic stroke due to arterial dissection
Abstract
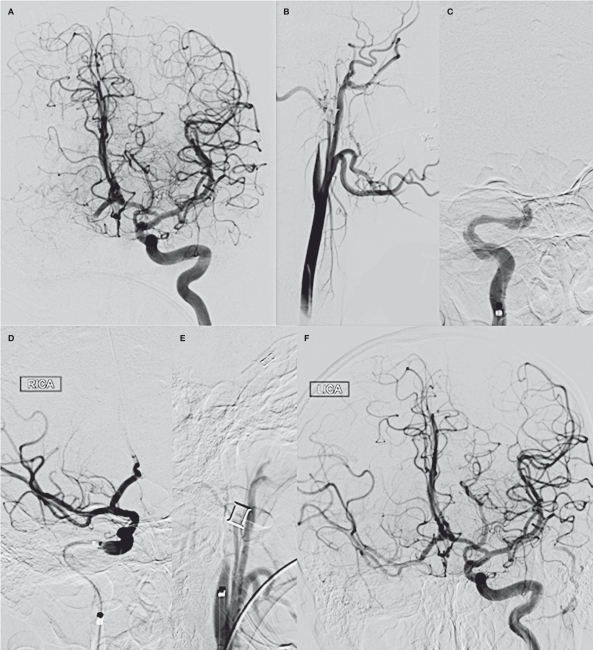
Arterial dissections account for 2% of strokes in all age groups, and up to 25% in patients aged 45 years or younger. The safety of endovascular intervention in this patient population is not well characterized. We identified all patients in the Merci registry - a prospective, multi-center post-market database enrolling patients treated with the Merci Retriever thrombectomy device - with arterial dissection as the most likely stroke etiology. Stroke presentation and procedural details were obtained prospectively; data regarding procedural complications, intracerebral hemorrhage (ICH), and the use of stenting of the dissected artery were obtained retrospectively. Of 980 patients in the registry, ten were identified with arterial dissection (8/10 ICA; 2/10 vertebrobasilar). The median age was 48 years with a baseline NIH stroke scale score of 16 and median time to treatment of 4.9 h. The procedure resulted in thrombolysis in cerebral ischemia (TICI) scores of 2a or better in eight out of ten and TICI 2b or better in six out of ten patients. Stenting of the dissection was performed in four of nine (44%). The single complication (1/9; 11%) - extension of a dissected carotid artery - was treated effectively with stenting. No symptomatic ICH or stroke in a previously unaffected territory occurred. A favorable functional outcome was observed in eight out of ten patients. Despite severe strokes on presentation, high rates of recanalization (8/10) and favorable functional outcomes (8/10) were observed. These results suggest that mechanical thrombectomy in patients with acute stroke resulting from arterial dissection is feasible, safe, and may be associated with favorable functional outcomes.
Figures
References
-
- Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. 2001;344:898–906. - PubMed
-
- Fava M, Meneses L, Loyola S, et al. Carotid artery dissection: endovascular treatment. Report of 12 patients. Catheter Cardiovasc Interv. 2008;71:694–700. - PubMed
-
- Pham MH, Rahme RJ, Arnaout O, et al. Endovascular stenting of extracranial carotid and vertebral artery dissections: a systematic review of the literature. Neurosurgery. 2011;68:856–866. discussion 866. - PubMed
-
- Yin Q, Li Y, Fan X, et al. Feasibility and safety of stenting for symptomatic carotid arterial dissection. Cerebrovasc Dis. 2011;32(Suppl 1):11–15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
