

Antenatal receipt of sulfadoxine-pyrimethamine does not exacerbate pregnancy-associated malaria despite the expansion of drug-resistant Plasmodium falciparum: clinical outcomes from the QuEERPAM study
- PMID: 22441649
- PMCID: PMC3520448
- DOI: 10.1093/cid/cis301
Antenatal receipt of sulfadoxine-pyrimethamine does not exacerbate pregnancy-associated malaria despite the expansion of drug-resistant Plasmodium falciparum: clinical outcomes from the QuEERPAM study
Abstract
Background: Antenatal intermittent preventive therapy with 2 doses of sulfadoxine-pyrimethamine (IPTp-SP) is the mainstay of efforts in sub-Saharan Africa to prevent pregnancy-associated malaria (PAM). Recent studies report that drug resistance may cause IPTp-SP to exacerbate PAM morbidity, raising fears that current policies will cause harm as resistance spreads.
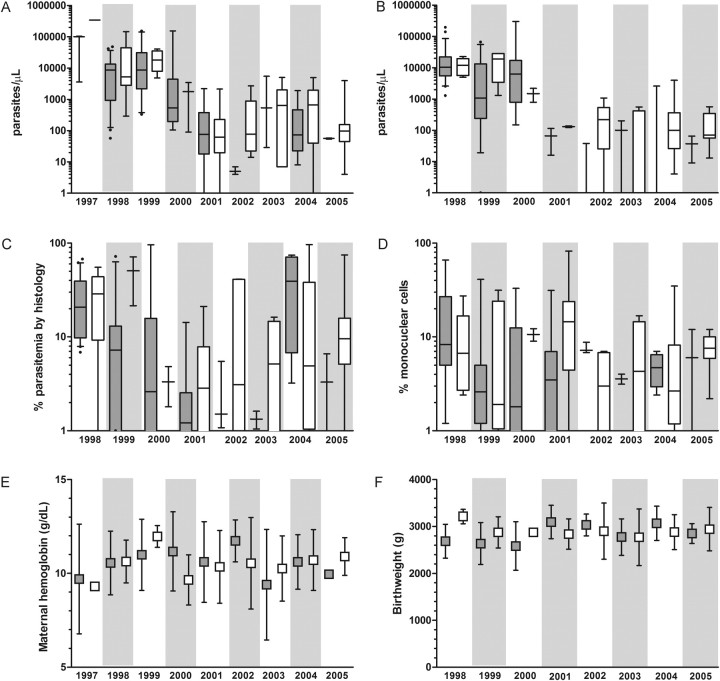
Methods: We conducted a serial, cross-sectional analysis of the relationships between IPTp-SP receipt, SP-resistant Plasmodium falciparum, and PAM morbidity in delivering women during a period of 9 years at a single site in Malawi. PAM morbidity was assessed by parasite densities, placental histology, and birth outcomes.
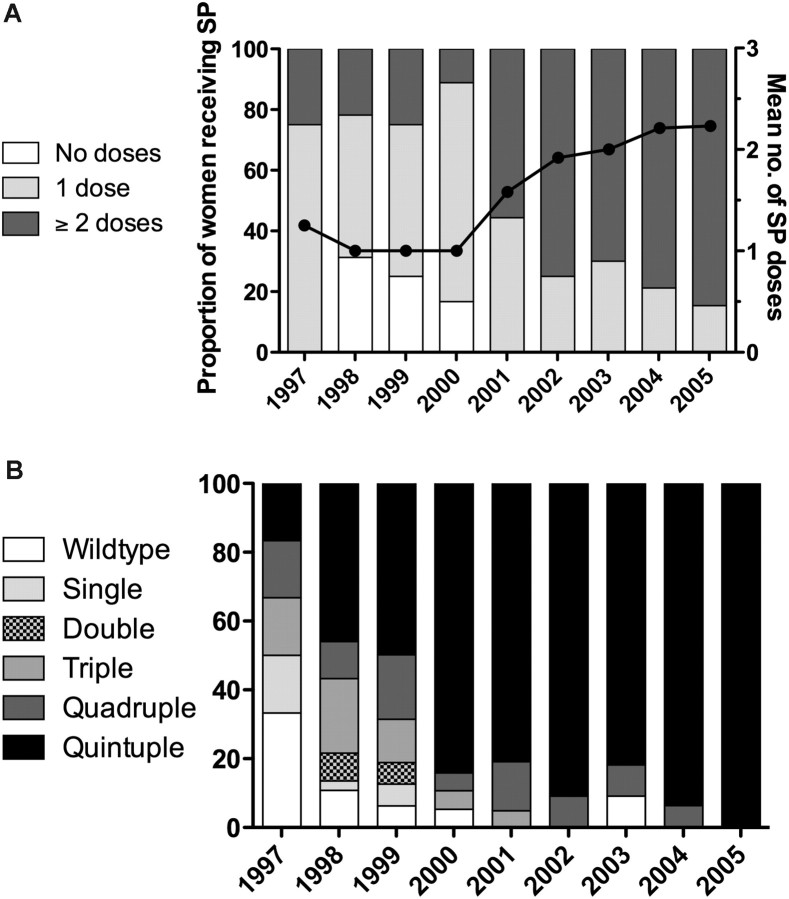
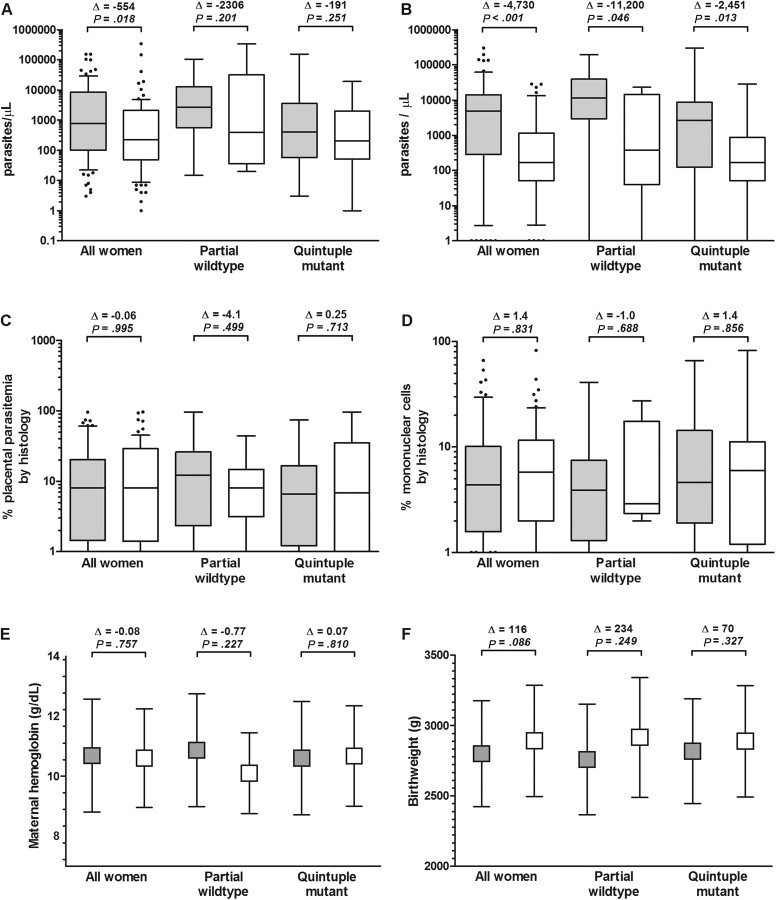
Results: The prevalence of parasites with highly SP-resistant haplotypes increased from 17% to 100% (P < .001), and the proportion of women receiving full IPTp (≥2 doses) increased from 25% to 82% (P < .001). Women who received full IPTp with SP had lower peripheral (P = .018) and placental (P < .001) parasite densities than women who received suboptimal IPTp (<2 doses). This effect was not significantly modified by the presence of highly SP-resistant haplotypes. After adjustment for covariates, the receipt of SP in the presence of SP-resistant P. falciparum did not exacerbate any parasitologic, histologic, or clinical measures of PAM morbidity.
Conclusions: In this longitudinal study of malaria at delivery, the receipt of SP as IPTp did not potentiate PAM morbidity despite the increasing prevalence and fixation of SP-resistant P. falciparum haplotypes. Even when there is substantial resistance, SP may be used in modified IPTp regimens as a component of comprehensive antenatal care.
Figures
Comment in
-
Intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine: the times they are a-changin'.Clin Infect Dis. 2012 Oct;55(7):1025-6; author reply 1026-7. doi: 10.1093/cid/cis568. Epub 2012 Jun 19. Clin Infect Dis. 2012. PMID: 22715177 No abstract available.
References
-
- Steketee RW, Nahlen BL, Parise ME, Menendez C. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64:28–35. - PubMed
-
- ter Kuile FO, van Eijk AM, Filler SJ. Effect of sulfadoxine-pyrimethamine resistance on the efficacy of intermittent preventive therapy for malaria control during pregnancy: a systematic review. JAMA. 2007;297:2603–16. - PubMed
-
- Sridaran S, McClintock SK, Syphard LM, Herman KM, Barnwell JW, Udhayakumar V. Anti-folate drug resistance in Africa: meta-analysis of reported dihydrofolate reductase (dhfr) and dihydropteroate synthase (dhps) mutant genotype frequencies in African Plasmodium falciparum parasite populations. Malar J. 2010;9:247. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
