

Topologically convergent and divergent structural connectivity patterns between patients with remitted geriatric depression and amnestic mild cognitive impairment
- PMID: 22442092
- PMCID: PMC6621223
- DOI: 10.1523/JNEUROSCI.5061-11.2012
Topologically convergent and divergent structural connectivity patterns between patients with remitted geriatric depression and amnestic mild cognitive impairment
Abstract
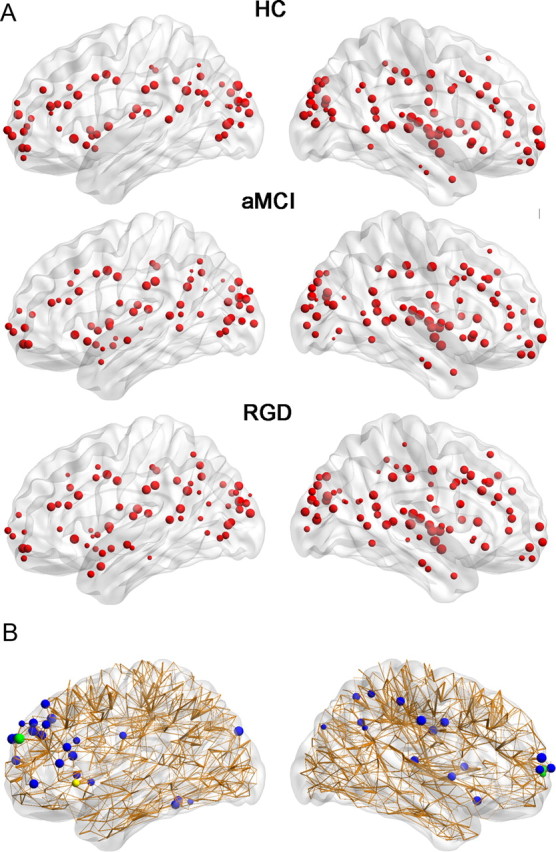
Alzheimer's disease (AD) can be conceptualized as a disconnection syndrome. Both remitted geriatric depression (RGD) and amnestic mild cognitive impairment (aMCI) are associated with a high risk for developing AD. However, little is known about the similarities and differences in the topological patterns of white matter (WM) structural networks between RGD and aMCI. In this study, diffusion tensor imaging and deterministic tractography were used to map the human WM networks of 35 RGD patients, 38 aMCI patients, and 30 healthy subjects. Furthermore, graph theoretical methods were applied to investigate the alterations in the global and regional properties of the WM network in these patients. First, both the RGD and aMCI patients showed abnormal global topology in their WM networks (i.e., reduced network strength, reduced global efficiency, and increased absolute path length) compared with the controls, and there were no significant differences in these global network properties between the patient groups. Second, similar deficits of the regional and connectivity characteristics in the WM networks were primarily found in the frontal brain regions of RGD and aMCI patients compared with the controls, while a different nodal efficiency of the posterior cingulate cortex and several prefrontal brain regions were also observed between the patient groups. Together, our study provides direct evidence for the association of a great majority of convergent and a minority of divergent connectivity of WM structural networks between RGD and aMCI patients, which may lead to increasing attention in defining a population at risk of AD.
Figures





References
-
- Alexopoulos GS, Murphy CF, Gunning-Dixon FM, Latoussakis V, Kanellopoulos D, Klimstra S, Lim KO, Hoptman MJ. Microstructural white matter abnormalities and remission of geriatric depression. Am J Psychiatry. 2008;165:238–244. - PubMed
-
- Bae JN, MacFall JR, Krishnan KR, Payne ME, Steffens DC, Taylor WD. Dorsolateral prefrontal cortex and anterior cingulate cortex white matter alterations in late-life depression. Biol Psychiatry. 2006;60:1356–1363. - PubMed
-
- Bai F, Zhang Z, Watson DR, Yu H, Shi Y, Yuan Y, Qian Y, Jia J. Abnormal integrity of association fiber tracts in amnestic mild cognitive impairment. J Neurol Sci. 2009a;278:102–106. - PubMed
-
- Bai F, Zhang Z, Watson DR, Yu H, Shi Y, Yuan Y, Zang Y, Zhu C, Qian Y. Abnormal functional connectivity of hippocampus during episodic memory retrieval processing network in amnestic mild cognitive impairment. Biol Psychiatry. 2009b;65:951–958. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical