

Unicystic ameloblastoma: A diagnostic dilemma
- PMID: 22442619
- PMCID: PMC3304231
- DOI: 10.4103/0975-5950.85863
Unicystic ameloblastoma: A diagnostic dilemma
Abstract
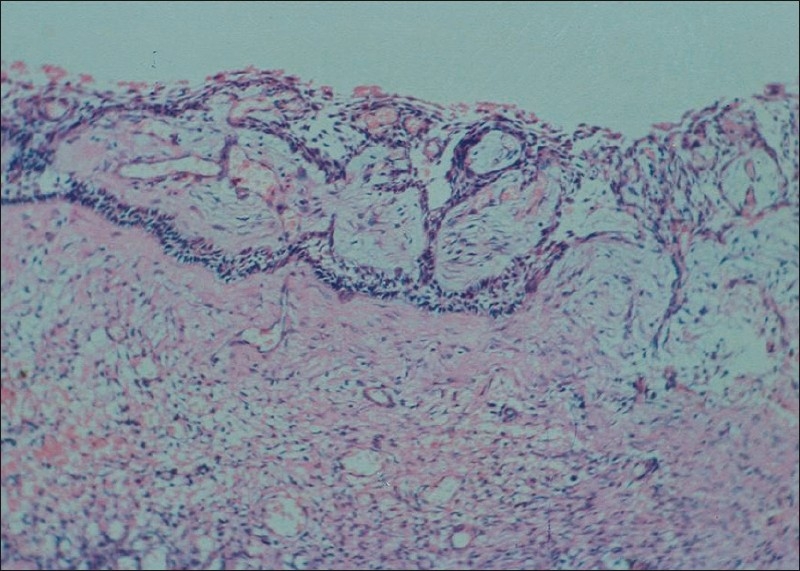
Ameloblastoma is a slow-growing, persistent and locally aggressive neoplasm of epithelial origin accounting for 10% out of 30% of all odontogenic tumors. According to the World Health Organization, ameloblastomas are classified into the following types: conventional, unicystic, and peripheral. Unicystic ameloblastoma (UA) refers to those cystic lesions that show clinical, radiographic, or gross features of a mandibular cyst, but on histologic examination show a typical ameloblastomatous epithelium lining part of the cyst cavity, with or without luminal and/or mural tumor growth. We report a case of young female with a radiolucent lesion in the right posterior mandible. Surgical removal of the lesion was performed, with differential diagnosis of a radicular cyst. However, histopathologic examination revealed UA. The patient was kept under observation and showed signs of local bone regeneration. The purpose of presenting this report of a clinical case of UA previously misdiagnosed as radicular cyst is to emphasize the significance of histopathologic examination of all tissue specimens recovered in surgery even when clinical and radiological finding are innocuous.
Keywords: Conservative treatment; radicular cyst; unicystic ameloblastoma.
Conflict of interest statement
Figures



References
-
- Gerzenshtein J, Zhang F, Caplan J, Anand V, Lineaweaver W. Immediate mandibular reconstruction with microsurgical fibula flap transfer following wide resection for ameloblastoma. J Craniofac Surg. 2006;17:178–82. - PubMed
-
- Philipsen HP, Reichart PA. London: Quintessence Pub Co Ltd; 2004. Classification of odontogenic tumors and allied lesions. Odontogenic tumors and allied lesions; pp. 21–3.
-
- Philipsen HP, Reichart PA. London: Quintessence Pub; 2004. Unicystic ameloblastoma. Odontogenic tumors and allied lesions; pp. 77–86.
-
- Leider AS, Eversole LR, Barkin ME. Cystic ameloblastoma: A clinicopathological analysis. Oral Surg Oral Med Oral Pathol. 1985;60:624–30. - PubMed
-
- Gardner DG, Corio RL. Plexiform unicystic ameloblastoma: Variant of ameloblastoma with a low recurrence rate after enucleation. Cancer. 1984;53:1730–5. - PubMed
