

Development of lung function in very low birth weight infants with or without bronchopulmonary dysplasia: longitudinal assessment during the first 15 months of corrected age
- PMID: 22443188
- PMCID: PMC3362756
- DOI: 10.1186/1471-2431-12-37
Development of lung function in very low birth weight infants with or without bronchopulmonary dysplasia: longitudinal assessment during the first 15 months of corrected age
Abstract
Background: Very low birth weight (VLBW) infants (< 1,500 g) with bronchopulmonary dysplasia (BPD) develop lung damage caused by mechanical ventilation and maturational arrest. We compared functional lung development after discharge from hospital between VLBW infants with and without BPD.
Methods: Comprehensive lung function assessment was performed at about 50, 70, and 100 weeks of postmenstrual age in 55 sedated VLBW infants (29 with former BPD [O2 supplementation was given at 36 weeks of gestational age] and 26 VLBW infants without BPD [controls]). Mean gestational age (26 vs. 29 weeks), birth weight (815 g vs. 1,125 g), and the proportion of infants requiring mechanical ventilation for ≥7 d (55% vs. 8%), differed significantly between BPD infants and controls.
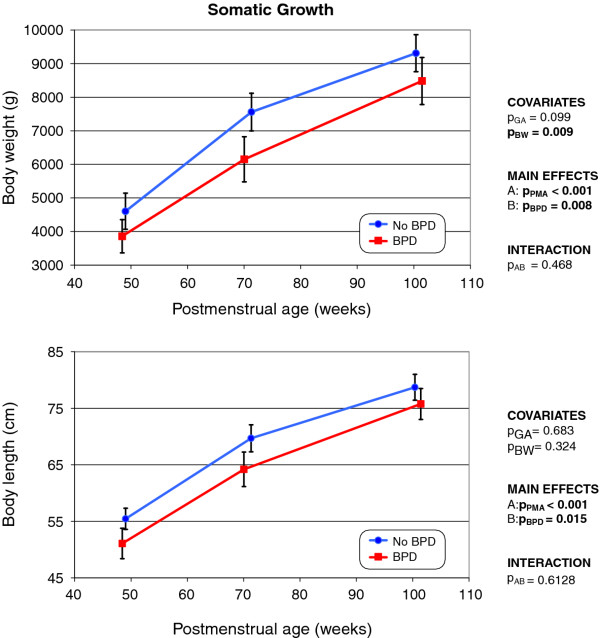
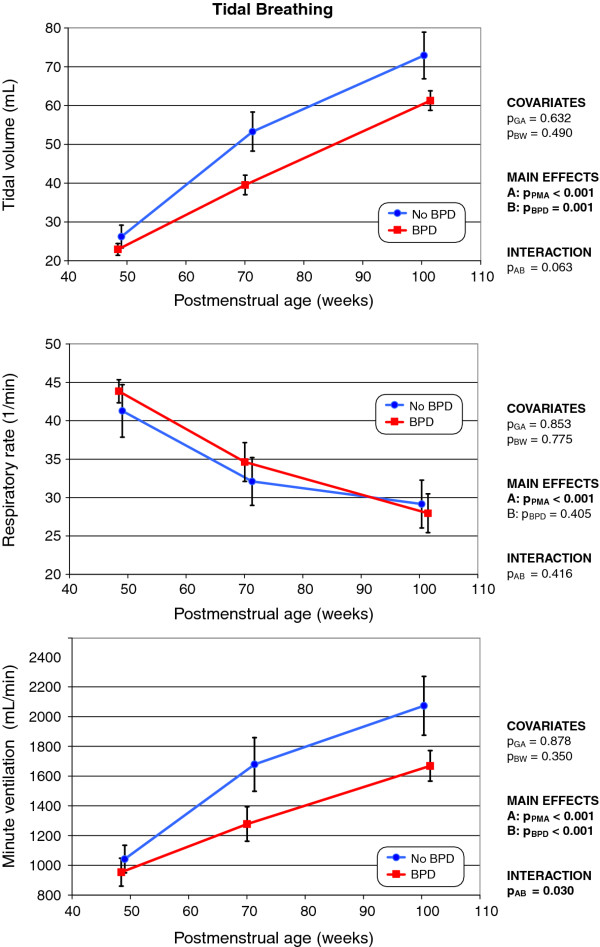
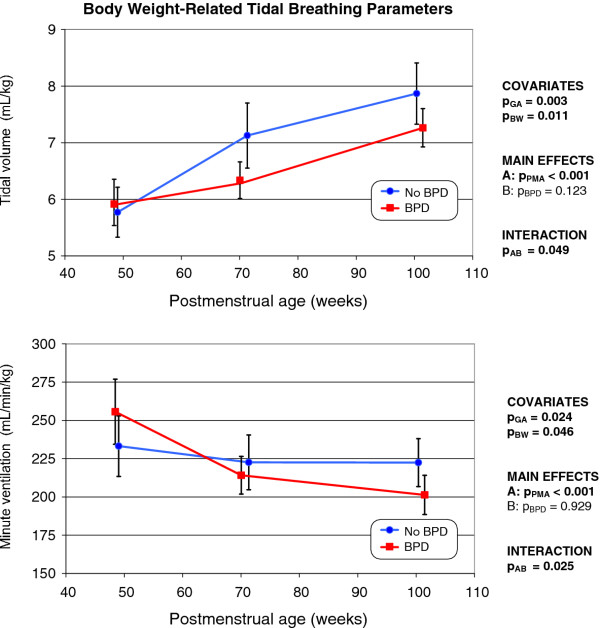
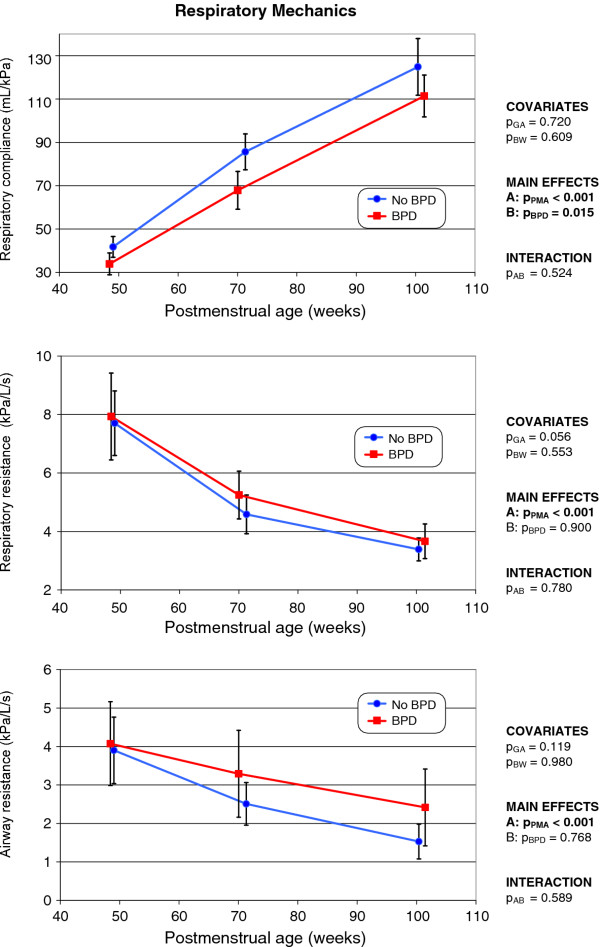
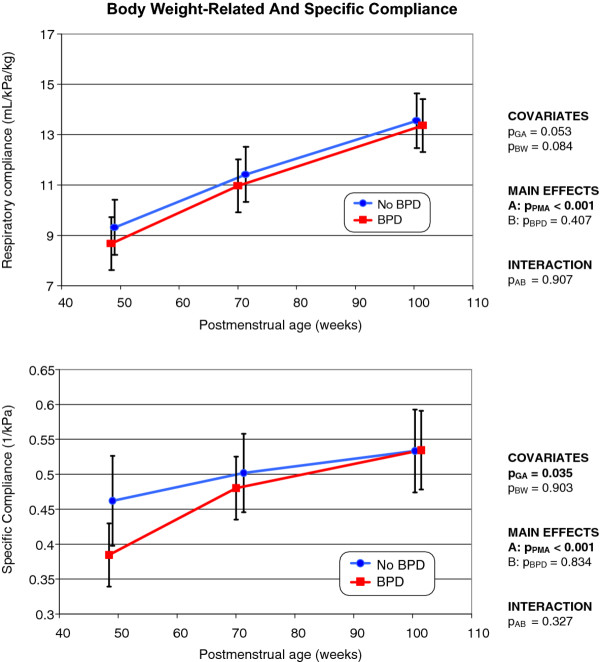
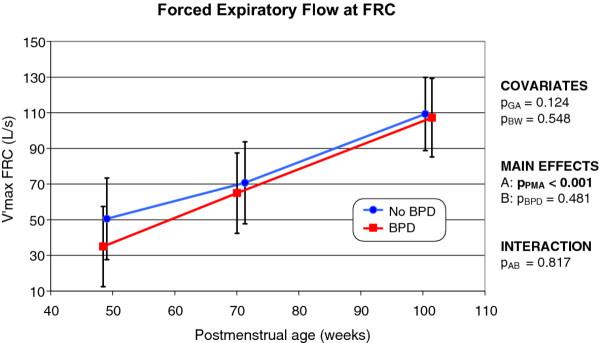
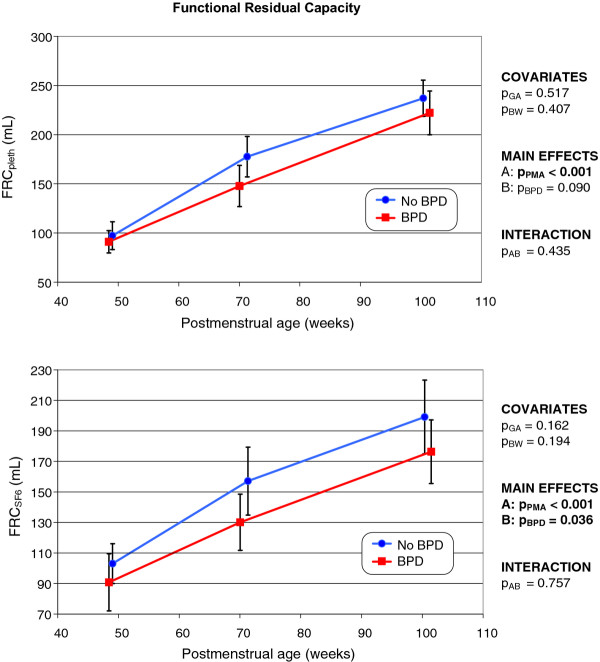
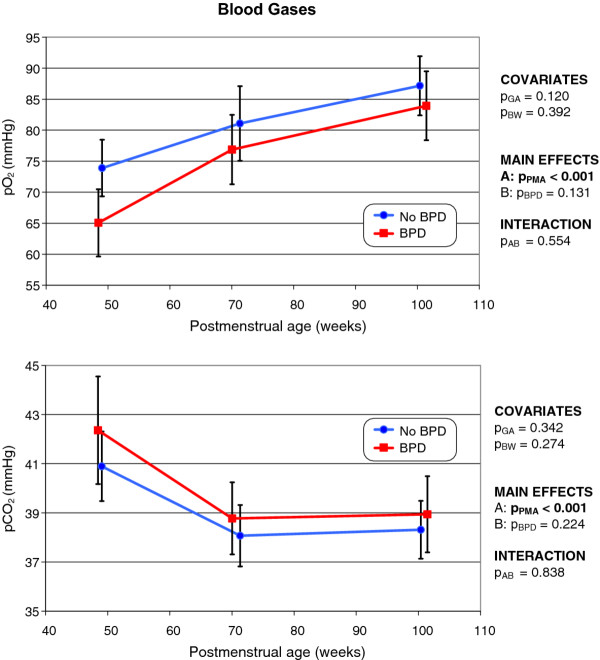
Results: Both body weight and length, determined over time, were persistently lower in former BPD infants compared to controls, but no significant between-group differences were noted in respiratory rate, respiratory or airway resistance, functional residual capacity as determined by body plethysmography (FRC(pleth)), maximal expiratory flow at the FRC (V'max (FRC)), or blood gas (pO2, pCO2) levels. Tidal volume, minute ventilation, respiratory compliance, and FRC determined by SF6 multiple breath washout (representing the lung volume in actual communication with the airways) were significantly lower in former BPD infants compared to controls. However, these differences became non-significant after normalization to body weight.
Conclusions: Although somatic growth and the development of some lung functional parameters lag in former BPD infants, the lung function of such infants appears to develop in line with that of non-BPD infants when a body weight correction is applied. Longitudinal lung function testing of preterm infants after discharge from hospital may help to identify former BPD infants at risk of incomplete recovery of respiratory function; such infants are at risk of later respiratory problems.
Figures
References
-
- Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR. et al.Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196:147–148. - PubMed
-
- Ramanathan R, Sardesai S. Lung protective ventilatory strategies in very low birth weight infants. J Perinatol. 2008;28(Suppl 1):S41–S46. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
