

Transport disposition using the Transport Risk Assessment in Pediatrics (TRAP) score
- PMID: 22443350
- PMCID: PMC3360797
- DOI: 10.3109/10903127.2012.664246
Transport disposition using the Transport Risk Assessment in Pediatrics (TRAP) score
Abstract
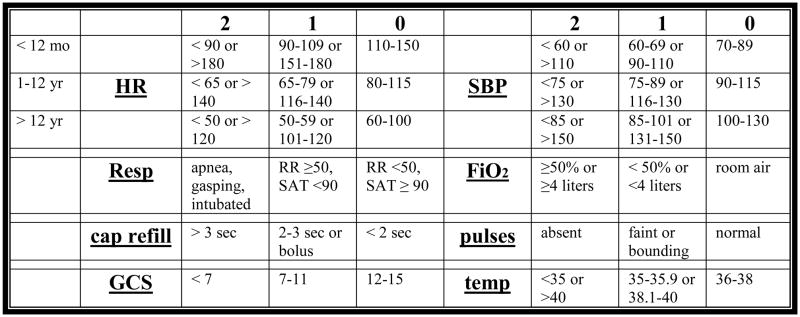
Background: Determining appropriate disposition for referred pediatric patients is difficult, since it relies primarily on a telephone description of the patient. In this study, we evaluate the Transport Risk Assessment in Pediatrics (TRAP) score's ability to assist in appropriate placement of these patients. This novel tool is derived from physiologic variables.
Objectives: To determine the feasibility of calculating a TRAP score and whether a higher score correlates with pediatric intensive care unit (PICU) admission.
Methods: We performed an observational study of pediatric patients transported by a specialized team to a tertiary care center and the feasibility of implementing the TRAP tool. Patients were eligible if transported by the pediatric specialty transport team for direct admission to the children's hospital. The TRAP score was obtained either through chart review of the transport team's initial assessment or in real time by the transport team.
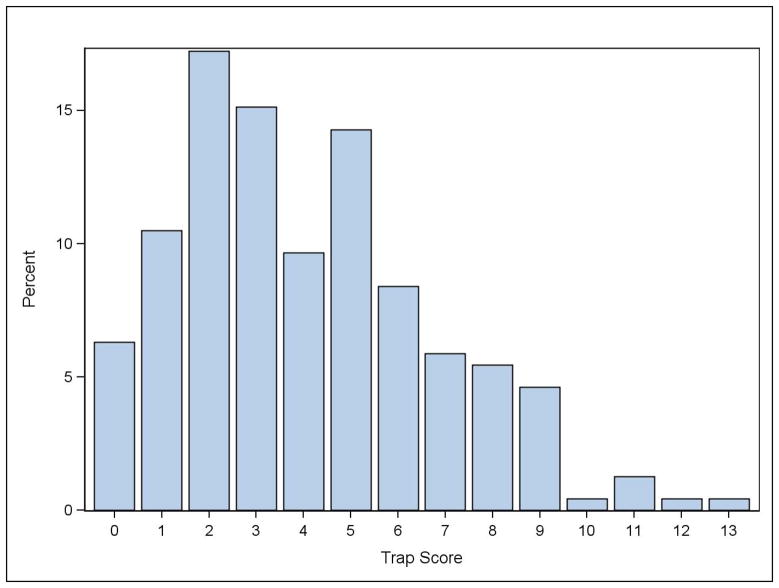
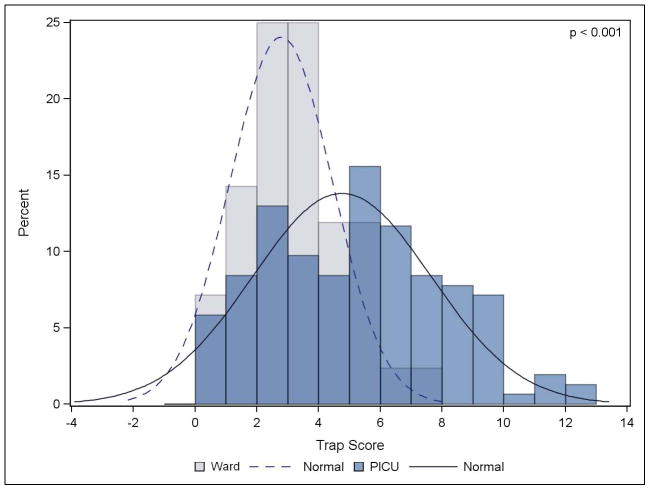
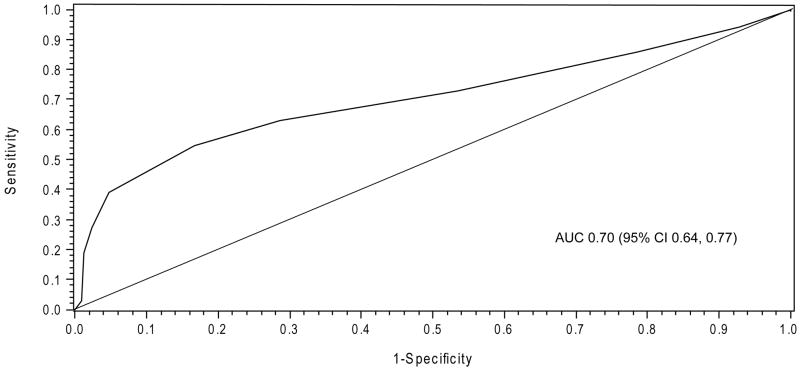
Results: A total of 269 patients were identified, with 238 patients included in the study. Using logistic regression, higher TRAP scores were associated with PICU admission (odds ratio [OR] 1.40, p < 0.001). Patients with a higher score were also less likely to leave the PICU within 24 hours (OR 0.79, p < 0.001).
Conclusion: The TRAP score is a novel objective pediatric transport assessment tool where an elevated score is associated with PICU admission for more than 24 hours. This score may assist with the triage decisions for transported pediatric patients.
Conflict of interest statement
Figures
References
-
- Usher RH. The role of the neonatologist. Pediatric Clinics of North America. 1970;17(1):199–202. - PubMed
-
- Swyer PR. The regional organisation of special care for the neonate. Pediatric Clinics of North America. 1970;17(4):761–776. - PubMed
-
- Pollack MM, Alexander SR, Clarke N, Ruttimann UE, Tesselaar HM, Bachulis AC. Improved outcomes from tertiary center pediatric intensive care: A statewide comparison of tertiary and nontertiary care facilities. Critical Care Medicine. 1991;19(2):150–159. - PubMed
-
- Perloff WH, Brill J, Ackerman A, Briglia F, Dimand R, Flores R, et al. Consensus report for regionalization of services for critically ill or injured children. Pediatrics. 2000;105(1 I):152–155. - PubMed
-
- Usher R. Changing mortality rates with perinatal intensive care and regionalization. Semin Perinatol. 1977;1(3):309–319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources