

Determinants of asthma after severe respiratory syncytial virus bronchiolitis
- PMID: 22444510
- PMCID: PMC3612548
- DOI: 10.1016/j.jaci.2012.02.010
Determinants of asthma after severe respiratory syncytial virus bronchiolitis
Abstract
Background: The development of asthma after respiratory syncytial virus (RSV) bronchiolitis has been demonstrated in case-control studies, although the determinants of post-RSV asthma remain undefined.
Objectives: We sought to evaluate the potential determinants of physician-diagnosed asthma after severe RSV bronchiolitis during infancy.
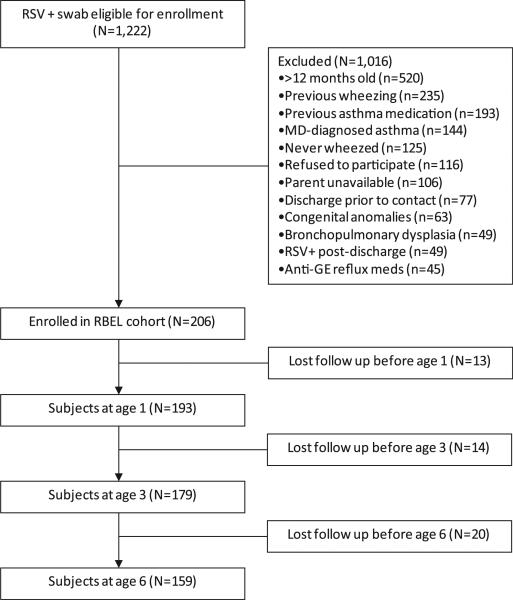
Methods: We enrolled 206 children during an initial episode of severe RSV bronchiolitis at 12 months of age or less in a prospective cohort study and followed these children for up to 6 years. In a subset of 81 children, we analyzed CCL5 (RANTES) mRNA expression in upper airway epithelial cells.
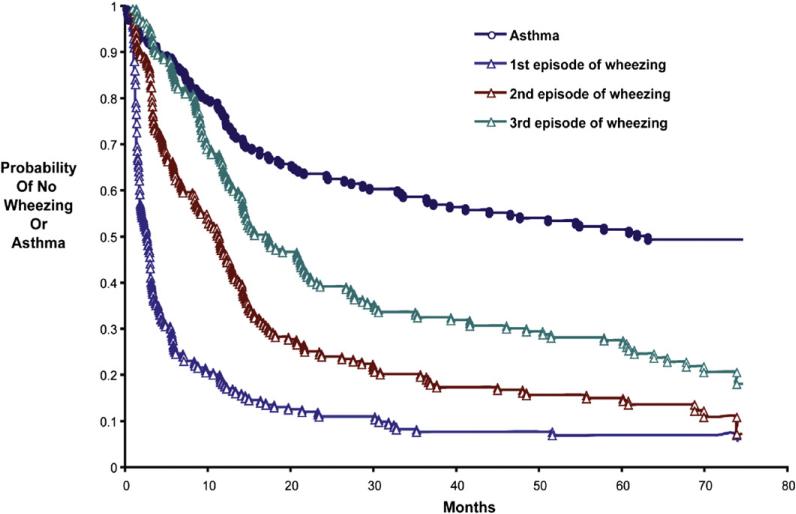
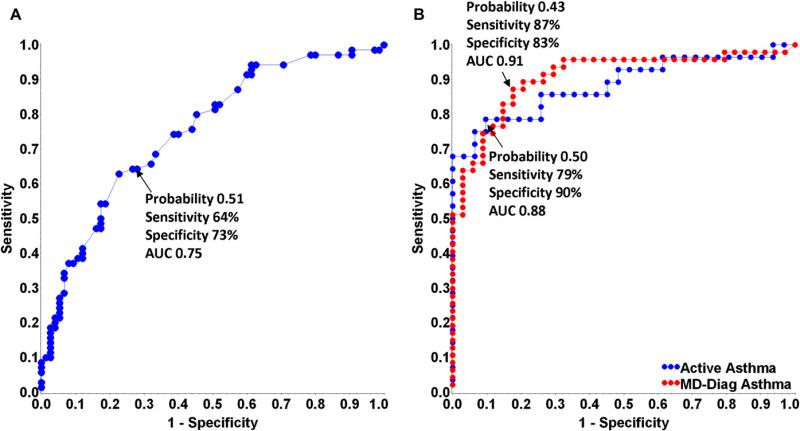
Results: Forty-eight percent of children had physician-diagnosed asthma before the seventh birthday. Independent determinants significantly associated with increased risk for physician-diagnosed asthma by the seventh birthday included maternal asthma (odds ratio [OR], 5.2; 95% CI, 1.7-15.9; P = .004), exposure to high levels of dog allergen (OR, 3.2; 95% CI, 1.3-7.7; P = .012), aeroallergen sensitivity at age 3 years (OR, 10.7; 95% CI, 2.1-55.0; P = .005), recurrent wheezing during the first 3 years of life (OR, 7.3; 95% CI, 1.2-43.3; P = .028), and CCL5 expression in nasal epithelia during acute RSV infection (OR, 3.8; 95% CI, 1.2-2.4; P < .001). White children (OR, 0.19; 95% CI, 0.04-0.93; P = .041) and children attending day care (OR, 0.18; 95% CI, 0.04-0.84; P = .029) had a decreased risk of physician-diagnosed asthma.
Conclusions: Approximately 50% of children who experience severe RSV bronchiolitis have a subsequent asthma diagnosis. The presence of increased CCL5 levels in nasal epithelia at the time of bronchiolitis or the development of allergic sensitization by age 3 years are associated with increased likelihood of subsequent asthma.
Copyright © 2012 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Why does respiratory syncytial virus appear to cause asthma?J Allergy Clin Immunol. 2012 Jul;130(1):101-2. doi: 10.1016/j.jaci.2012.05.024. J Allergy Clin Immunol. 2012. PMID: 22742838 No abstract available.
References
-
- Glezen WP, Taber LH, Frank AL, Kasel JA. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1986;140:543–6. - PubMed
-
- Leader S, Kohlhase K. Respiratory syncytial virus-coded pediatric hospitalizations, 1997 to 1999. Pediatr Infect Dis J. 2002;21:629–32. - PubMed
-
- Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am J Respir Crit Care Med. 2000;161:1501–7. - PubMed
-
- Schauer U, Hoffjan S, Bittscheidt J, Kochling A, Hemmis S, Bongartz S, et al. RSV bronchiolitis and risk of wheeze and allergic sensitisation in the first year of life. Eur Respir J. 2002;20:1277–83. - PubMed
-
- Henderson J, Hilliard TN, Sherriff A, Stalker D, Al Shammari N, Thomas HM. Hospitalization for RSV bronchiolitis before 12 months of age and subsequent asthma, atopy and wheeze: a longitudinal birth cohort study. Pediatr Allergy Immunol. 2005;16:386–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
