

Hemoglobin-driven pathophysiology is an in vivo consequence of the red blood cell storage lesion that can be attenuated in guinea pigs by haptoglobin therapy
- PMID: 22446185
- PMCID: PMC3314461
- DOI: 10.1172/JCI59770
Hemoglobin-driven pathophysiology is an in vivo consequence of the red blood cell storage lesion that can be attenuated in guinea pigs by haptoglobin therapy
Abstract
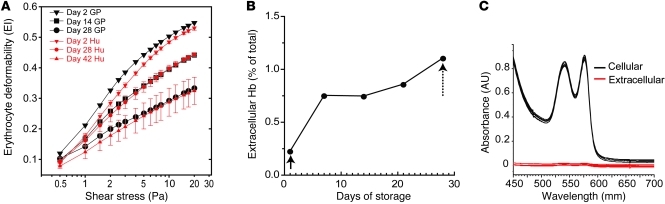
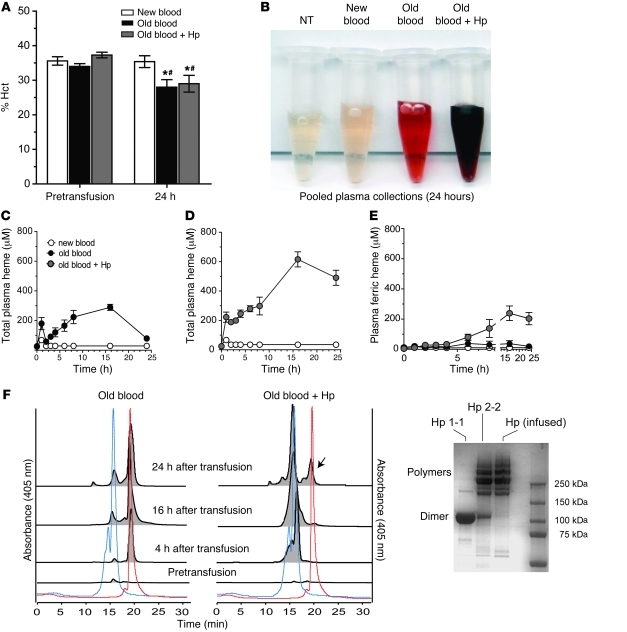
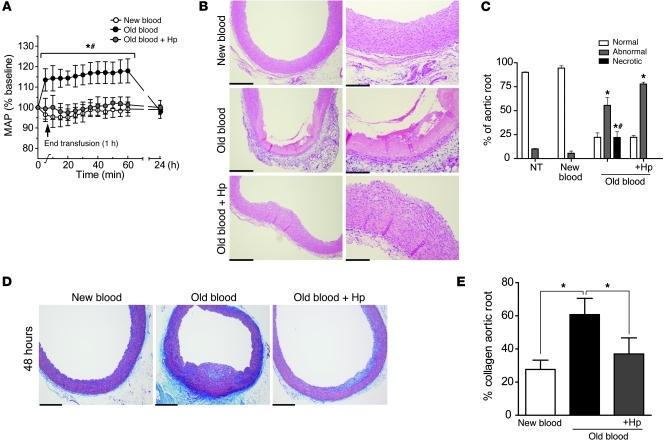
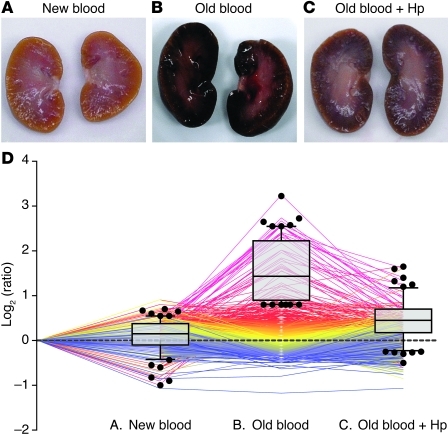
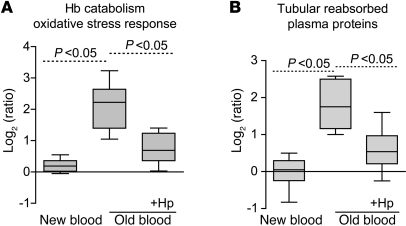
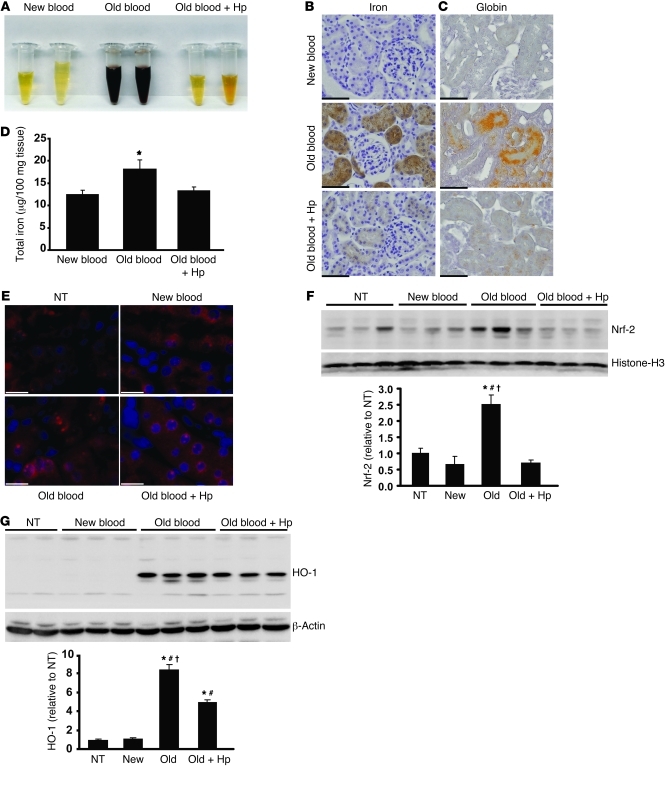
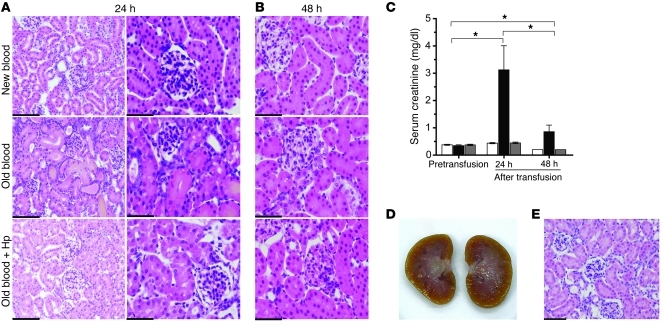
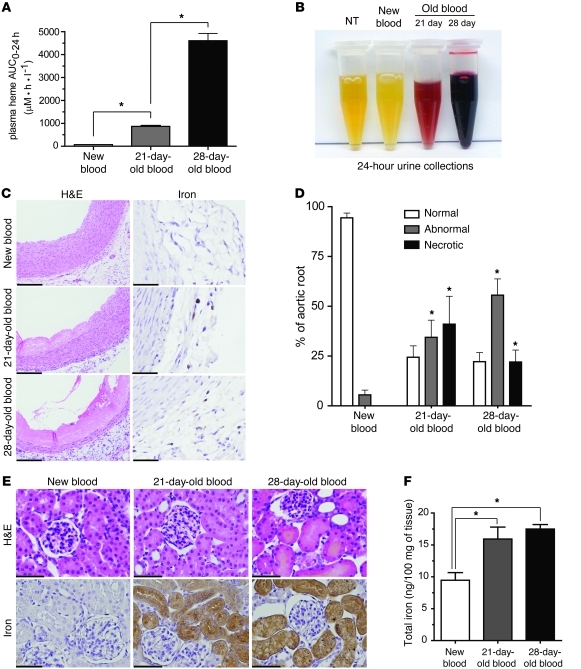
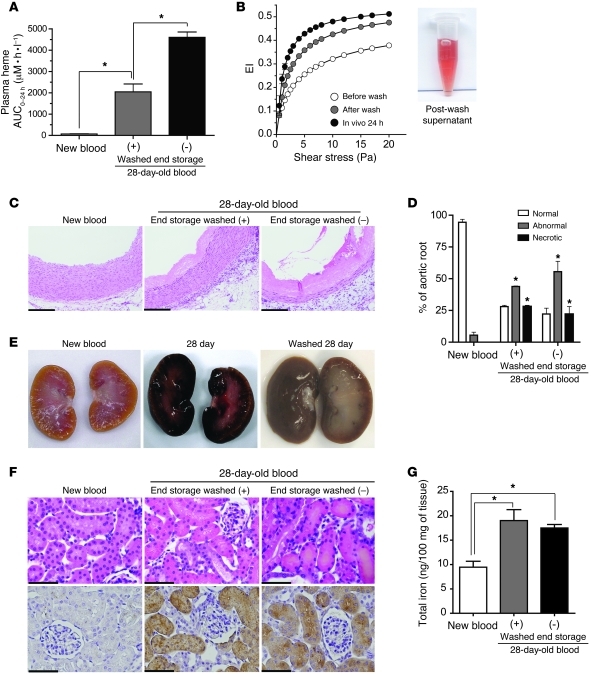
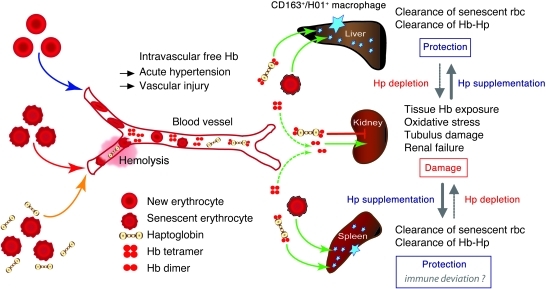
Massive transfusion of blood can lead to clinical complications, including multiorgan dysfunction and even death. Such severe clinical outcomes have been associated with longer red blood cell (rbc) storage times. Collectively referred to as the rbc storage lesion, rbc storage results in multiple biochemical changes that impact intracellular processes as well as membrane and cytoskeletal properties, resulting in cellular injury in vitro. However, how the rbc storage lesion triggers pathophysiology in vivo remains poorly defined. In this study, we developed a guinea pig transfusion model with blood stored under standard blood banking conditions for 2 (new), 21 (intermediate), or 28 days (old blood). Transfusion with old but not new blood led to intravascular hemolysis, acute hypertension, vascular injury, and kidney dysfunction associated with pathophysiology driven by hemoglobin (Hb). These adverse effects were dramatically attenuated when the high-affinity Hb scavenger haptoglobin (Hp) was administered at the time of transfusion with old blood. Pathologies observed after transfusion with old blood, together with the favorable response to Hp supplementation, allowed us to define the in vivo consequences of the rbc storage lesion as storage-related posttransfusion hemolysis producing Hb-driven pathophysiology. Hb sequestration by Hp might therefore be a therapeutic modality for enhancing transfusion safety in severely ill or massively transfused patients.
Figures
Comment in
-
Hemolysis and cell-free hemoglobin drive an intrinsic mechanism for human disease.J Clin Invest. 2012 Apr;122(4):1205-8. doi: 10.1172/JCI62972. Epub 2012 Mar 26. J Clin Invest. 2012. PMID: 22446184 Free PMC article.
References
-
- Haradin AR, Weed RI, Reed CF. Changes in physical properties of stored erythrocytes relationship to survival in vivo. Transfusion. 1969;9(5):229–237. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
