

Clinical and cost effectiveness of mobile phone supported self monitoring of asthma: multicentre randomised controlled trial
- PMID: 22446569
- PMCID: PMC3311462
- DOI: 10.1136/bmj.e1756
Clinical and cost effectiveness of mobile phone supported self monitoring of asthma: multicentre randomised controlled trial
Abstract
Objective: To determine whether mobile phone based monitoring improves asthma control compared with standard paper based monitoring strategies.
Design: Multicentre randomised controlled trial with cost effectiveness analysis.
Setting: UK primary care.
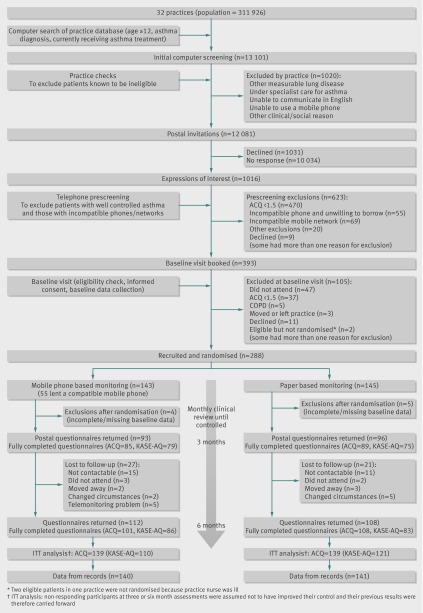
Participants: 288 adolescents and adults with poorly controlled asthma (asthma control questionnaire (ACQ) score ≥ 1.5) from 32 practices.
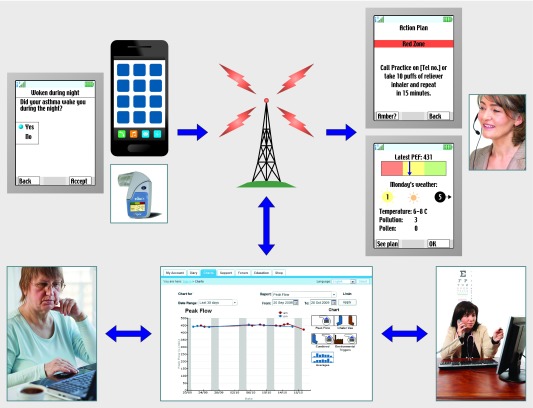
Intervention: Participants were centrally randomised to twice daily recording and mobile phone based transmission of symptoms, drug use, and peak flow with immediate feedback prompting action according to an agreed plan or paper based monitoring.
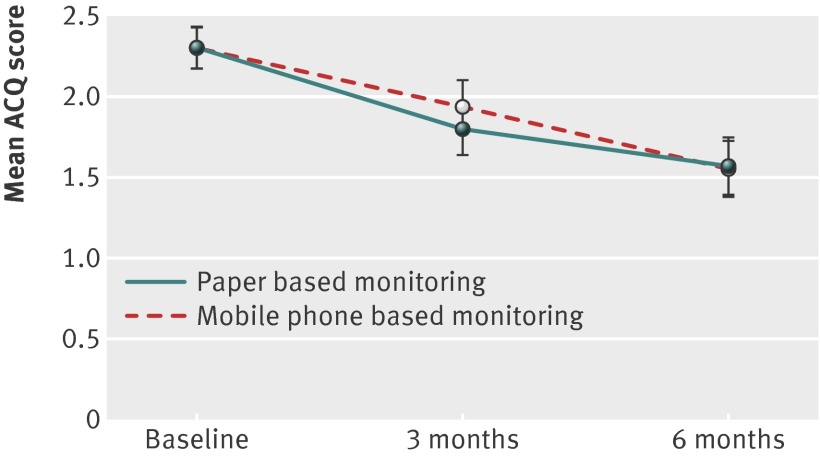
Main outcome measures: Changes in scores on asthma control questionnaire and self efficacy (knowledge, attitude, and self efficacy asthma questionnaire (KASE-AQ)) at six months after randomisation. Assessment of outcomes was blinded. Analysis was on an intention to treat basis.
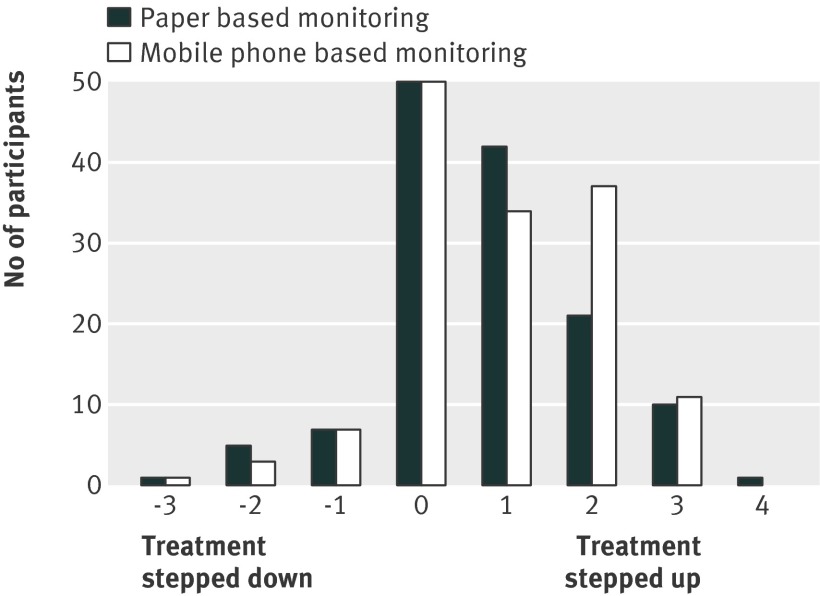
Results: There was no significant difference in the change in asthma control or self efficacy between the two groups (ACQ: mean change 0.75 in mobile group v 0.73 in paper group, mean difference in change -0.02 (95% confidence interval -0.23 to 0.19); KASE-AQ score: mean change -4.4 v -2.4, mean difference 2.0 (-0.3 to 4.2)). The numbers of patients who had acute exacerbations, steroid courses, and unscheduled consultations were similar in both groups, with similar healthcare costs. Overall, the mobile phone service was more expensive because of the expenses of telemonitoring.
Conclusions: Mobile technology does not improve asthma control or increase self efficacy compared with paper based monitoring when both groups received clinical care to guidelines standards. The mobile technology was not cost effective.
Trial registration: Clinical Trials NCT00512837.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma. Global Initiative for Asthma, 2003. www.ginasthma.com. - PubMed
-
- McIvor RA, Chapman KR. The coming of age of asthma guidelines. Lancet 2008;372:1021-2. - PubMed
-
- Rabe KF, Adachi M, Lai CK, Soriano JB, Vermeire PA, Weiss KB, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol 2004;114:40-7. - PubMed
-
- Campbell S, Reeves D, Kontopantelis E, Middleton E, Sibbald B, Roland M. Quality of primary care in England with the introduction of pay for performance. N Engl J Med 2007;357:181-90. - PubMed
-
- Gibson PG, Powell H, Wilson A, Abramson MJ, Haywood P, Bauman A, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2002;3:CD001117. - PubMed