

The effects of QEEG-informed neurofeedback in ADHD: an open-label pilot study
- PMID: 22446998
- PMCID: PMC3419351
- DOI: 10.1007/s10484-012-9191-4
The effects of QEEG-informed neurofeedback in ADHD: an open-label pilot study
Abstract
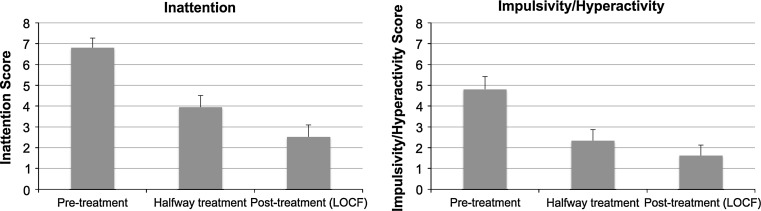
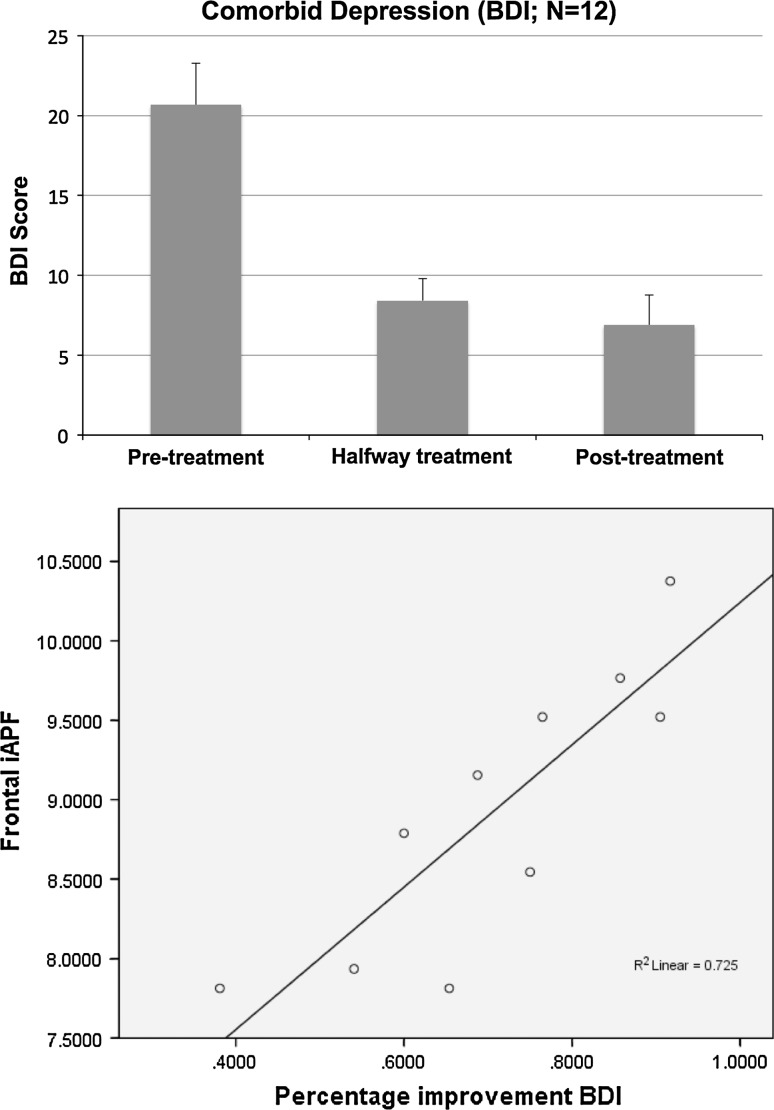
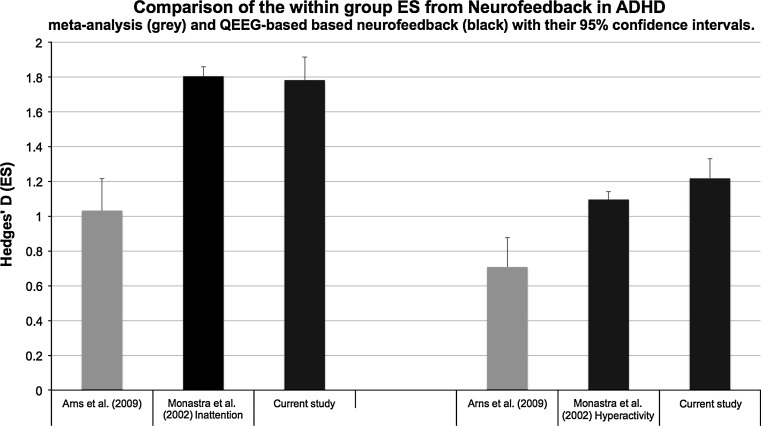
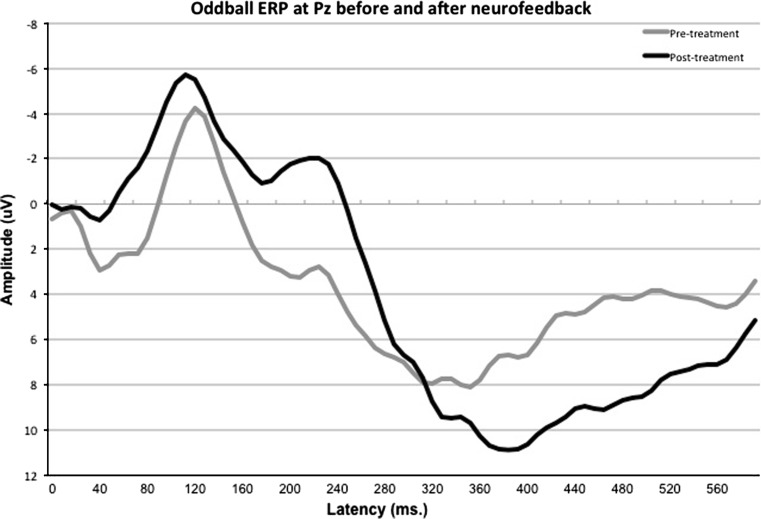
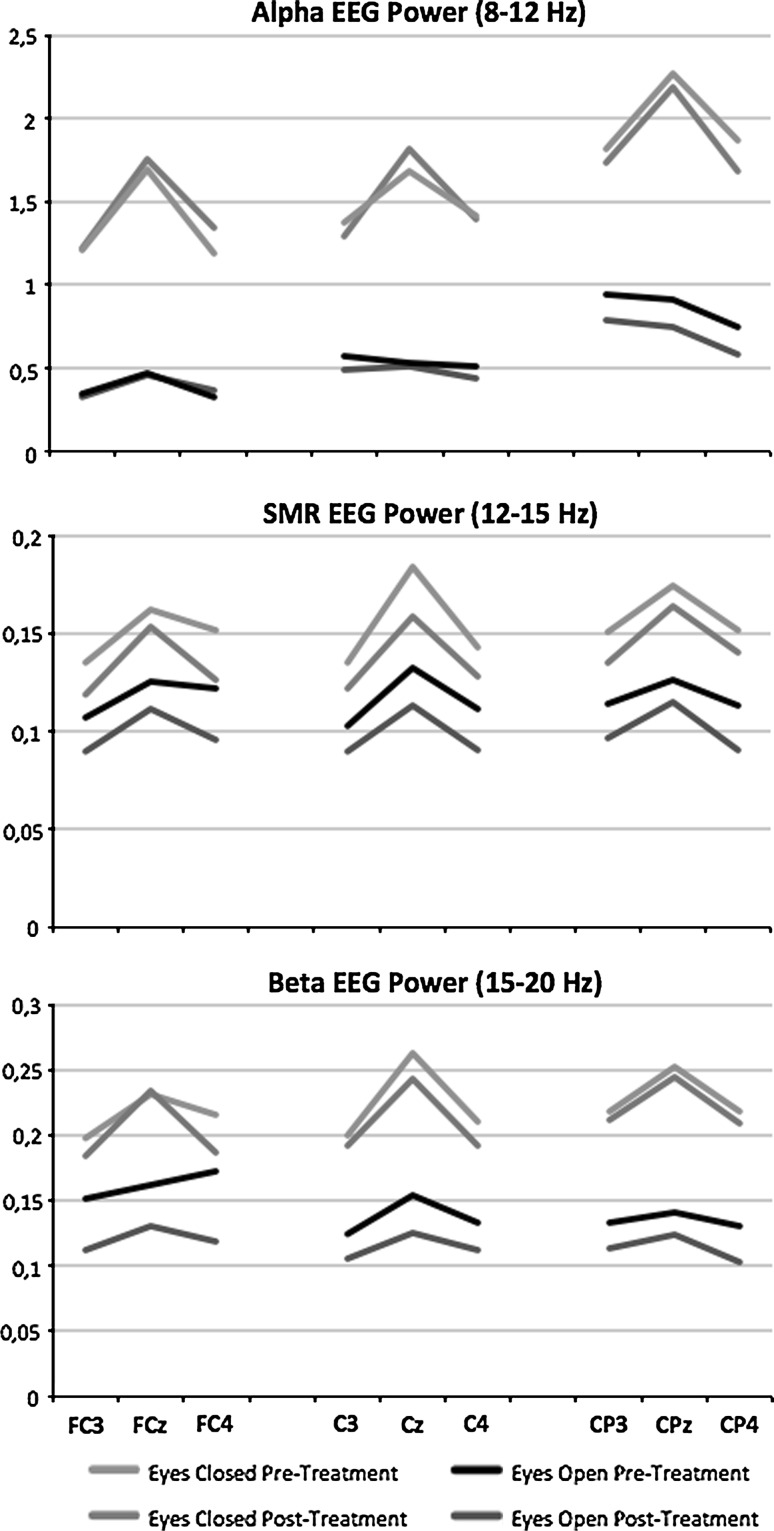
In ADHD several EEG biomarkers have been described before, with relevance to treatment outcome to stimulant medication. This pilot-study aimed at personalizing neurofeedback treatment to these specific sub-groups to investigate if such an approach leads to improved clinical outcomes. Furthermore, pre- and post-treatment EEG and ERP changes were investigated in a sub-group to study the neurophysiological effects of neurofeedback. Twenty-one patients with ADHD were treated with QEEG-informed neurofeedback and post-treatment effects on inattention (ATT), hyperactivity/impulsivity (HI) and comorbid depressive symptoms were investigated. There was a significant improvement for both ATT, HI and comorbid depressive complaints after QEEG-informed neurofeedback. The effect size for ATT was 1.78 and for HI was 1.22. Furthermore, anterior individual alpha peak frequency (iAPF) demonstrated a strong relation to improvement on comorbid depressive complaints. Pre- and post-treatment effects for the SMR neurofeedback sub-group exhibited increased N200 and P300 amplitudes and decreased SMR EEG power post-treatment. This pilot study is the first study demonstrating that it is possible to select neurofeedback protocols based on individual EEG biomarkers and suggests this results in improved treatment outcome specifically for ATT, however these results should be replicated in further controlled studies. A slow anterior iAPF at baseline predicts poor treatment response on comorbid depressive complaints in line with studies in depression. The effects of SMR neurofeedback resulted in specific ERP and EEG changes.
Figures
References
-
- Arns, M., Drinkenburg, W. H. I. M., Fitzgerald, P. B., & Kenemans, J. L. (in press). Neurophysiological predictors of non-response to rTMS in depression. Brain Stimulation. doi:10.1016/j.brs.2011.12.003. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
