

Management of acute coronary syndrome in South Africa: insights from the ACCESS (Acute Coronary Events - a Multinational Survey of Current Management Strategies) registry
- PMID: 22447241
- PMCID: PMC3721828
- DOI: 10.5830/CVJA-2012-017
Management of acute coronary syndrome in South Africa: insights from the ACCESS (Acute Coronary Events - a Multinational Survey of Current Management Strategies) registry
Abstract
Background: The burden of cardiovascular diseases is predicted to escalate in developing countries. While many studies have reported the descriptive epidemiology, practice patterns and outcomes of patients hospitalised with acute coronary syndromes (ACS), these have largely been confined to the developed nations.
Methods: In this prospective, observational registry, 12 068 adults hospitalised with a diagnosis of ACS were enrolled between January 2007 and January 2008 at 134 sites in 19 countries in Africa, Latin America and the Middle East. Data on patient characteristics, treatment and outcomes were collected.
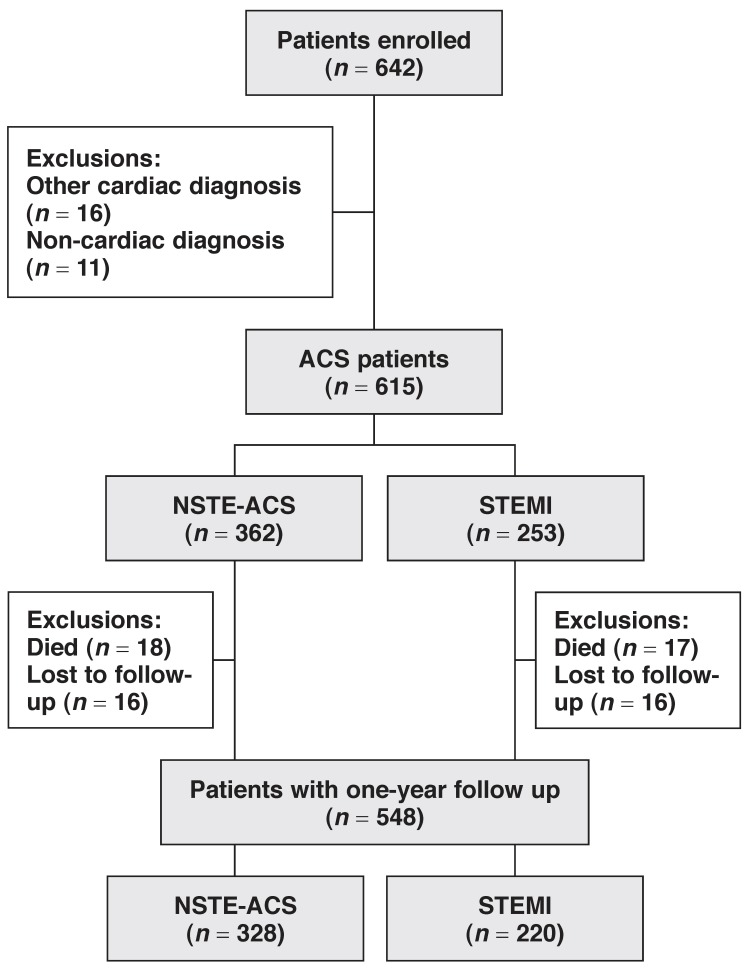
Results: Of the 642 patients from South Africa in the registry, 615 had a confirmed ACS diagnosis and form the basis of this report; 41% had a discharge diagnosis of ST-segment elevation myocardial infarction (STEMI) and 59% a diagnosis of non-ST-segment elevation acute coronary syndrome (NSTE-ACS), including 32% with non-ST-segment elevation myocardial infarction (NSTEMI) and 27% with unstable angina (UA). During hospitalisation, most patients received aspirin (94%) and a lipid-lowering medication (91%); 69% received a beta-blocker, and 66% an ACE inhibitor/angiotensin receptor blocker. Thrombolytic therapy was used in only 18% of subjects (36% of STEMI patients and 5.5% of NSTE-ACS patients). Angiography was undertaken in 93% of patients (61.3% on the first day), of whom 53% had a percutaneous coronary intervention (PCI) and 14% were referred for coronary artery bypass surgery. Drug-eluting stents were used in 57.9% of cases. Clopidogrel was prescribed at discharge from hospital in 62.2% of patients. All-cause death at 12 months was 5.7%, and was higher in patients with STEMI versus non-ST-elevation ACS (6.7 vs 5.0%, p < 0.0001). Clinical factors associated with higher risk of death at 12 months included age ≥ 70 years, presence of diabetes mellitus on admission, and a history of stroke/transient ischaemic attack (TIA).
Conclusions: In this observational study of ACS patients, the use of evidence-based pharmacological therapies for ACS was quite high. Interventional rates were high compared to international standards, and in particular the use of drug-eluting stents, yet the clinical outcomes (mortality, re-admission rates and severe bleeding episodes at one year) were favourable, with low rates compared with other studies.
References
-
- Kumar A, Fonarow GC, Eagle KA, Hirsch AT, Califf RM, Alberts MJ. et al. Regional and practice variation in adherence to guideline recommendations for secondary and primary prevention among out-patients with atherothrombosis or risk factors in the United States: a report from the REACH Registry. Crit Path Cardiol. 2009;8(3):104–11. - PubMed
-
- Eagle KA, Goodman SG, Avezum A, Budaj A, Sullivan CM, Lopez-Sendon J. Practice variation and missed opportunities for reperfusion in ST-segment-elevation myocardial infarction: findings from the Global Registry of Acute Coronary Events (GRACE). Lancet. 2002;359(9304):373–377. - PubMed
-
- Fox KA, Goodman SG, Anderson FA Jr, Granger CB, Moscucci M, Flather MD. et al. From guidelines to clinical practice: the impact of hospital and geographical characteristics on temporal trends in the management of acute coronary syndromes. The Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2003;24(15):1414–1424. - PubMed
-
- Patel MR, Chen AY, Roe MT, Ohman EM, Newby LK, Harrington RA. et al. A comparison of acute coronary syndrome care at academic and nonacademic hospitals. Am J Med. 2007;120(1):40–46. - PubMed
-
- Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U. EUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur J Cardiovasc Prev Rehabil. 2009;16(2):121–137. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
