

Tuberculosis spine: Therapeutically refractory disease
- PMID: 22448055
- PMCID: PMC3308658
- DOI: 10.4103/0019-5413.93685
Tuberculosis spine: Therapeutically refractory disease
Abstract
Background: India ranks second amongst the high-burden multi drug resistant tuberculosis (MDR-TB) countries, with an estimated incidence of 2.3% MDR-TB cases amongst the new cases and 17.2% amongst the previously treated cases. The diagnosis and treatment protocol for MDR-TB of the spine are not clearly established. We report outcome of a series of 15 cases of TB spine who were suspected to be therapeutically refractory cases (MDR-TB) on the basis of clinicoradiological failures of initial treatment.
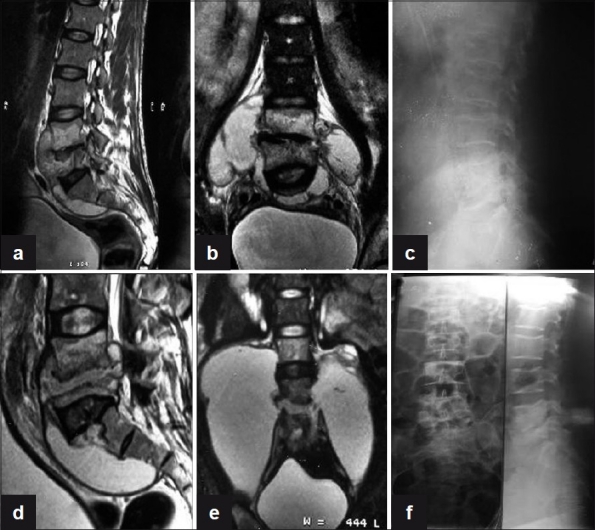
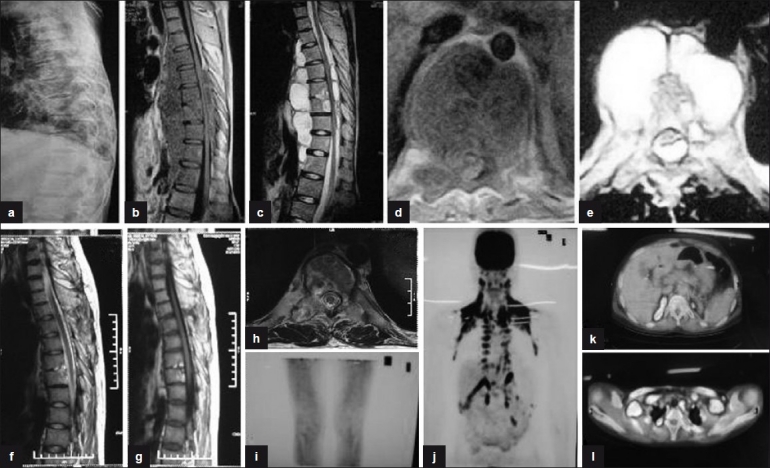
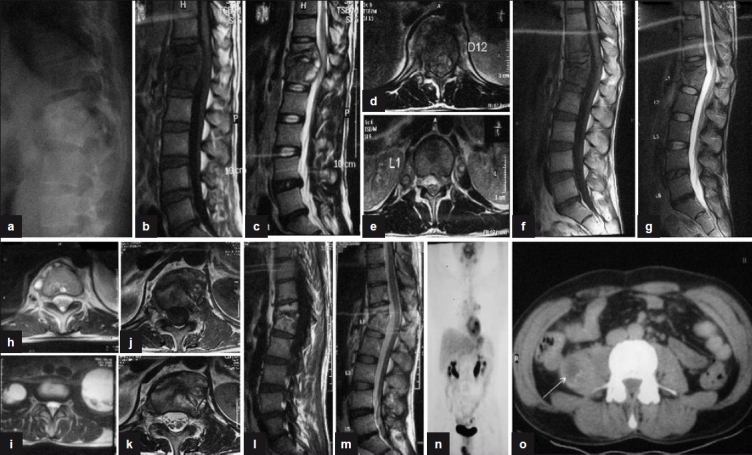
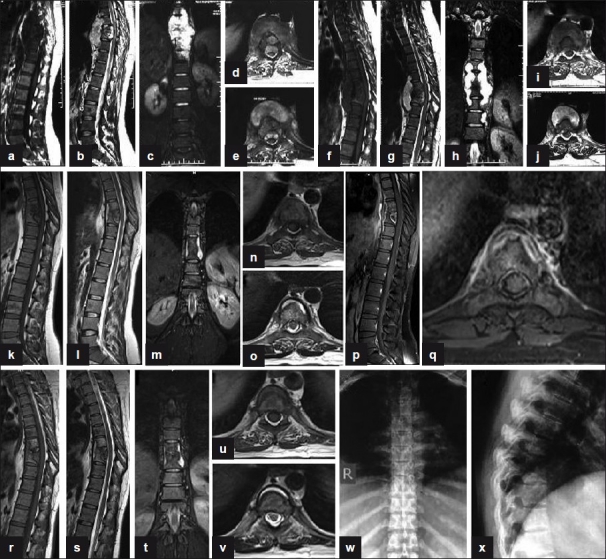
Materials and methods: Fifteen cases of TB spine from C2 to L5 spine were suspected to be the cases of MDR-TB (therapeutically refractory cases) on the basis of failures of adequate clinicoradiological healing response at 5 months or more on antitubercular treatment (ATT). None of the patient was immunocompromised. Thirteen out of 15 patients had tissue samples sent for histopathology, culture and sensitivity, smear, BACTEC, and polymerase chain reaction (PCR). All patients were put on second line ATT and followed up fortnightly with regular liver and kidney function tests, erythrocyte sedimentation rate (ESR), and plain X-ray. Healing was documented as subjective improvement of symptoms, reduction in ESR, and observations on contrast enhanced magnetic resonance imaging (MRI) such as resolution of marrow edema, fatty replacement of bone marrow and resolution of abscesses. Ambiguous MRI observations in a few patients were resolved on positron emission tomography (PET) scan. Patients were monitored continuously for 2 years after stopping ATT.
Results: We could demonstrate a positive culture in three cases. Two of them had multi drug resistance. We could achieve healing status in 13 out of 14 patients after starting second line drugs, one patient is still on treatment while other patient with no drug resistance is responding well on ATT.
Conclusions: The suspicion of therapeutically refractory case is of paramount importance. Once suspected, surgery to procure tissue for diagnosis and culture is to be undertaken. The demonstration of drug resistance on culture may not be achieved in all TB spine cases and empiric drug regimen for MDR-TB is to be started. We have achieved the healed status with immunomodulation and second line ATT. The length of treatment needs to be monitored with MRI and PET scan.
Keywords: MRI; TB spine; multi drug resistance; therapeutically refractory disease.
Conflict of interest statement
Figures
References
-
- The World Health Organization/International Union Against Tuberculosis and Lung Disease (WHO/UNION) Global Project on Anti-Tuberculosis Drug Resistance Surveillance 2002–2007 Anti-Tuberculosis Drug Resistance In The World: Fourth Global Report
-
- Park K. 21st ed. Jabalpur, India: M/s Banarsidas Bhanot Publishers; 2011. Park textbook of preventive and social medicine; p. 164.
-
- Pyle MM. Relative numbers of resistant tubercle bacilli in sputum of patients before and during treatment with streptomycin. Proc Mayo Clin. 1947;22:465–73. - PubMed
-
- Tuli SM. Challenge of therapeutically refractory and multidrug resistant tuberculosis in orthopaedic practice. Indian J Orthop. 2002;36:211–3.
LinkOut - more resources
Full Text Sources
Miscellaneous