

Tuberculosis of hip in children: A retrospective analysis
- PMID: 22448058
- PMCID: PMC3308661
- DOI: 10.4103/0019-5413.93686
Tuberculosis of hip in children: A retrospective analysis
Abstract
Background: Tuberculosis (TB) of hip constitutes nearly 15% of all cases of osteoarticular tuberculosis. We report a retrospective study carried out on 43 children with hip TB.
Materials and methods: Forty-three children of TB hip treated between 1971 and 2000 were analysed. Twenty-four children of the early series were treated with streptomycin (S), isoniazid (H) and PAS (Pa) for 18 months (3HPaS, 15 HPa), while 19 children in the later series were treated with isoniazid (H), rifampicin (R) and ethambutol (E) or pyrazinamide (Z) for 12 months [(12 RHE(Z)]. Five out of 18 children with radiologically normal appearing type hip TB were treated with chemotherapy alone and 38 children were subjected to surgery; simple synovectomy alone in 31 hips, joint debridement in six hips, and proximal femoral varisation osteotomy in one. After surgery hips were immobilized in cast for one to three months according to the severity of the disease and patients pain tolerance, and then were mobilized under leg traction in bed gradually till pain subsided completely.
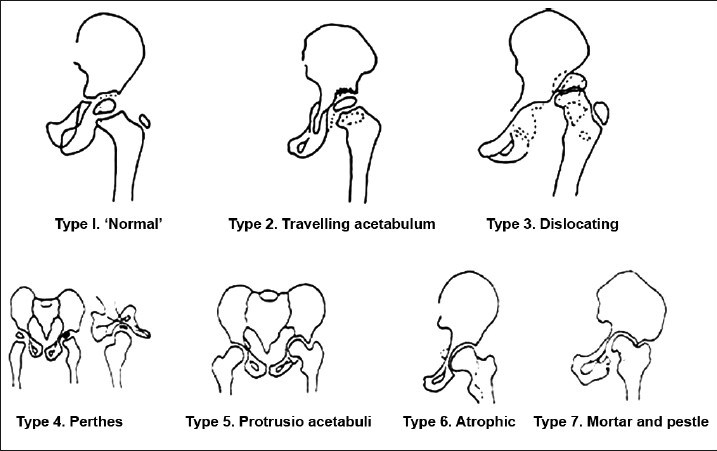
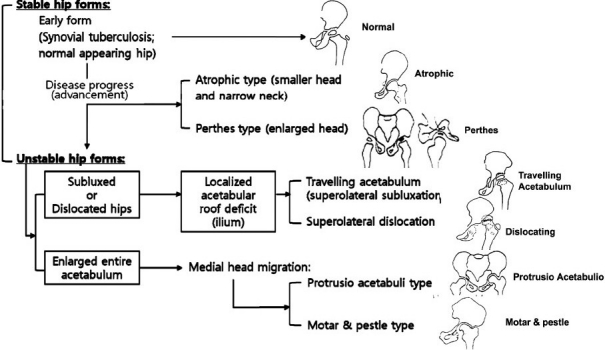
Results: TB of hip healed with minimum sequelae in all children. In 18 Type one hip TB, normal hip (synovial form) anatomy was maintained, and in 25 patients with advanced lesions some defect in the femoral head and acetabulum was noticed, though painless good hip motion was maintained. Excellent to good results were obtained in 31 children (73.1%), fair in eight (18.6%), and poor in four (9.3%). In four patients with poor results, there was some residual morphological defect in the hip. None developed ankylosis of hip.
Conclusion: We achieved good outcome with minimum sequelae in this series. The management goal should be aimed not only to heal the disease but also to maintain a painless mobile hip and anatomical cephalocotyloid relationship until maturity, and retard the development of secondary osteoarthritis.
Keywords: Tuberculosis; hip; infective arthritis; osteoarticular.
Conflict of interest statement
Figures




References
-
- Babhulkar S, Pande S. Tuberculosis of the hip. Clin Orthop Relat Res. 2002;398:93–9. - PubMed
-
- Campbell JA, Hoffman EB. Tuberculosis of the hip in children. J Bone Joint Surg Br. 1995;77:319–26. - PubMed
-
- Shanmugasundaram TK. A clinicoradiological classification of tuberculosis of the hip. In: Shanmugasundaram TK, editor. Current concepts in bone and joint tuberculosis. Madras, India: Proceedings of Combined Congress of International Bone and Joint Tuberculosis Club and the Indian Orthop Assoc; 1983. p. 60.
-
- Vora PH. Role of early surgery in management of tuberculosis of hip. In: Shanmugasundaram TK, editor. Current concept in bone and joint tuberculosis. Madras, India: Proceedings of Combined Congress of International Bone and Joint Tuberculosis Clue and the Indian Orthopedic Association; 1983. p. 60.
-
- Metha MT. Prognosis of tuberculous arthritis. In: Shanmugasundaram TK, editor. ibi-dem. Chennai: 1983. pp. 78–80.
LinkOut - more resources
Full Text Sources
Miscellaneous