

Giant cell tumors of the axial skeleton
- PMID: 22448122
- PMCID: PMC3289906
- DOI: 10.1155/2012/410973
Giant cell tumors of the axial skeleton
Abstract
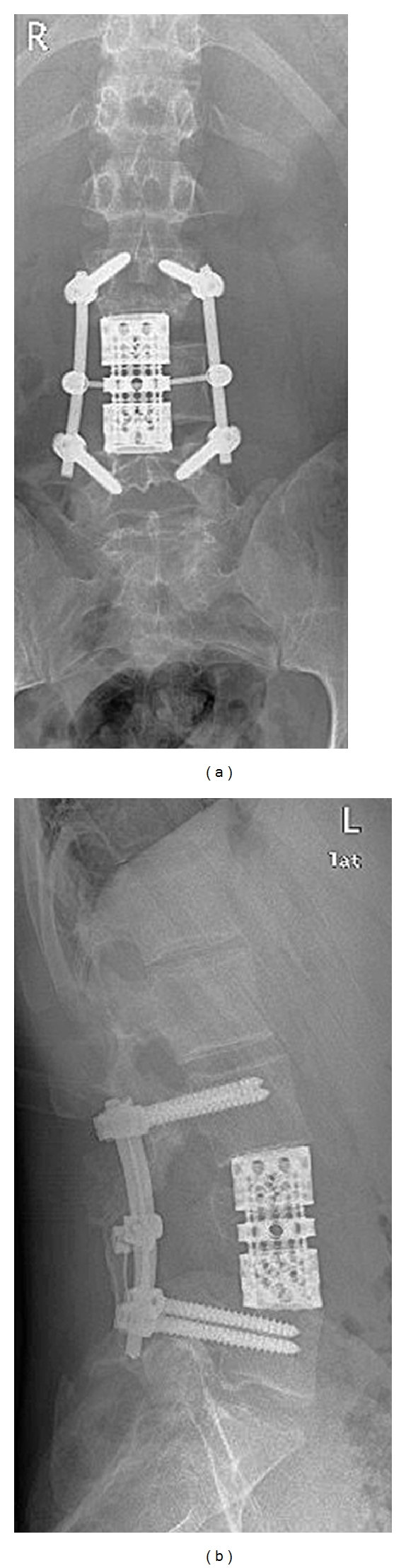
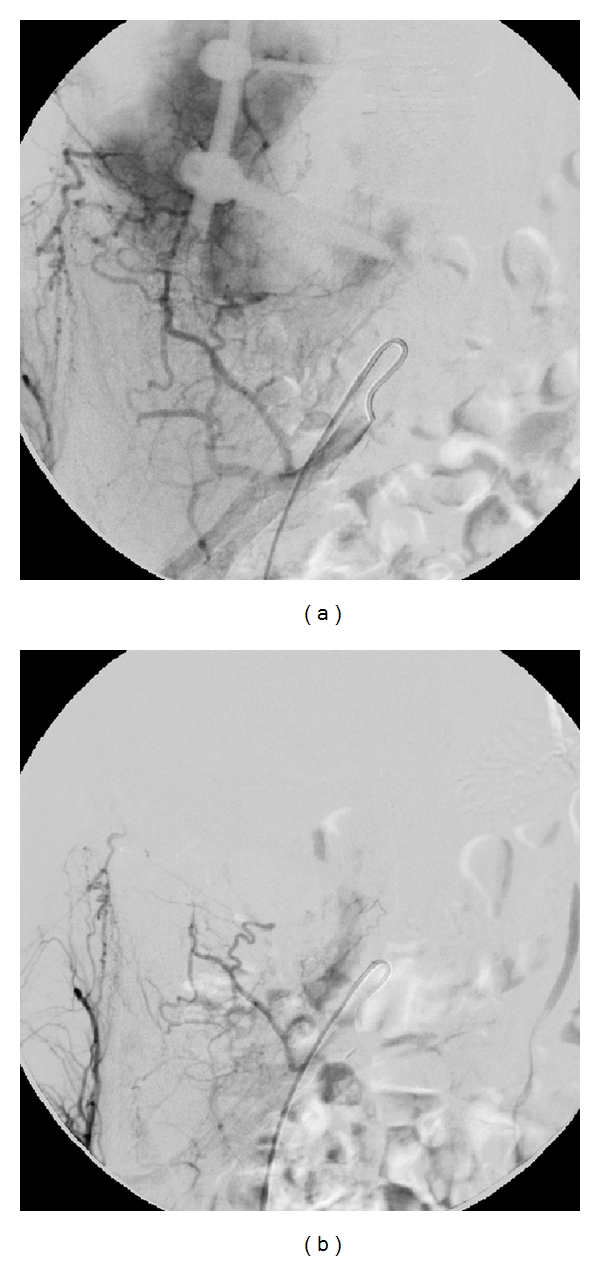
Background. We report on 19 cases of giant cell tumor of bone (GCT) affecting the spine or sacrum and evaluate the outcome of different treatment modalities. Methods. Nineteen patients with GCT of the spine (n = 6) or sacrum (n = 13) have been included in this study. The mean followup was 51.6 months. Ten sacral GCT were treated by intralesional procedures of which 4 also received embolization, and 3 with irradiation only. All spinal GCT were surgically treated. Results. Two (15.4%) patients with sacral and 4 (66.7%) with spinal tumors had a local recurrence, two of the letter developed pulmonary metastases. One local recurrence of the spine was successfully treated by serial arterial embolization, a procedure previously described only for sacral tumors. At last followup, 9 patients had no evidence of disease, 8 had stable disease, 1 had progressive disease, 1 died due to disease. Six patients had neurological deficits. Conclusions. GCT of the axial skeleton have a high local recurrence rate. Neurological deficits are common. En-bloc spondylectomy combined with embolization is the treatment of choice. In case of inoperability, serial arterial embolization seems to be an alternative not only for sacral but also for spinal tumors.
Figures

References
-
- Balke M, Schremper L, Gebert C, et al. Giant cell tumor of bone: treatment and outcome of 214 cases. Journal of Cancer Research and Clinical Oncology. 2008;134(9):969–978. - PubMed
-
- Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. Journal of Bone and Joint Surgery. Series A. 1987;69(1):106–114. - PubMed
-
- Freyschmidt J, Ostertag H, Jundt G. Knochentumoren. 2. Auflage. Berlin, Germany: Springer; 1998.
-
- Carrasco CH, Murray JA. Giant cell tumors. Orthopedic Clinics of North America. 1989;20(3):395–405. - PubMed
-
- Salzer-Kuntschik M. Differential diagnosis of giant cell tumor of bone. Verhandlungen der Deutschen Gesellschaft für Pathologie. 1998;82:154–159. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
