

doi: 10.1155/2012/816541.
Epub 2012 Feb 9.
Imaging diagnosis of interstitial pneumonia with emphysema (combined pulmonary fibrosis and emphysema)
Affiliations
- PMID: 22448329
- PMCID: PMC3289947
- DOI: 10.1155/2012/816541
Item in Clipboard
Imaging diagnosis of interstitial pneumonia with emphysema (combined pulmonary fibrosis and emphysema)
Pulm Med.
2012.
Abstract
Based on clinical and radiological findings, Cottin defined combined pulmonary fibrosis and emphysema (CPFE) as pulmonary emphysema in the upper lungs and interstitial pneumonia in the lower lungs with various radiological patterns. Pathologic findings of CPFE probably corresponded with diffuse interstitial pneumonia with pulmonary emphysema, emphysema with fibrosis, and the combination of both. We described reported radiological findings of CPFE.
Figures
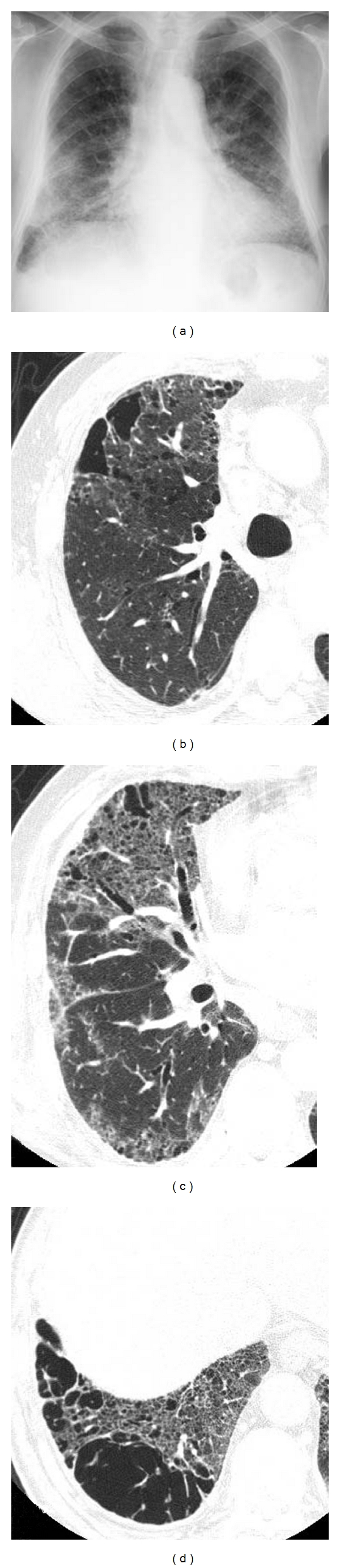
Diffuse interstitial pneumonia (nonspecific interstitial pneumonia (NSIP) pattern) with emphysema. (a) Chest X-ray shows bibasilar ground glass and reticular opacity. Volumes of bilateral lungs are almost normal. (b) High-resolution computed tomography (HRCT) of upper lung shows centrilobular pulmonary emphysema. (c), (d) HRCT of lower lung shows ground glass opacity along the bronchovascular bundle including cysts with varying size. Distribution of abnormal opacity mimics NSIP.
Diffuse interstitial pneumonia (UIP pattern) with emphysema. (a) Chest X-ray shows decreased volume of bilateral lungs. Ground glass opacity including reticular opacity and honeycomb lung in bilateral lower lungs. (b) HRCT of the right upper lobe shows paraseptal emphysema in ventral aspect. (c) HRCT of the right lower lobe shows ground glass opacity and honeycomb lung. Traction bronchiectasis is also observed within the areas of honeycombing.

Diffuse interstitial pneumonia (UIP pattern), emphysema with fibrosis. The patient underwent right lower lobectomy for lung cancer of the right lower lobe. (a) HRCT of the right upper lobe shows severe centrilobular emphysema. (b) HRCT of the right lower lobe shows slight ground glass opacity including several thick-walled cyst. (c) HRCT of basilar region shows subpleural ground glass opacity and reticular opacity in the subpleural region: radiologically consistent with UIP pattern. There are some relatively thick-walled cysts in subpleural region; however, no evidence of honeycombing. (d) Pathologic specimen (H&E staining) shows centrilobular and paraseptal emphysema with collagen type fibrosis. (e) Pathologic specimen shows dense centrilobular collagen-type fibrosis, associated with centrilobular emphysema. (f) Pathologic specimen shows cystic lesion in the acinus with destruction of alveoli and dense perilobular and peribronchiolar fibrosis. Normal alveoli adjacent to the cystic lesion. (g) Pathologic specimen shows patchy subpleural and intralobular fibrosis with alternating emphysematous, nonfibrotic area. Note fibroblastic foci (arrows). Sharp border between advanced fibrosis and normally appeared tissue suggests UIP pattern.

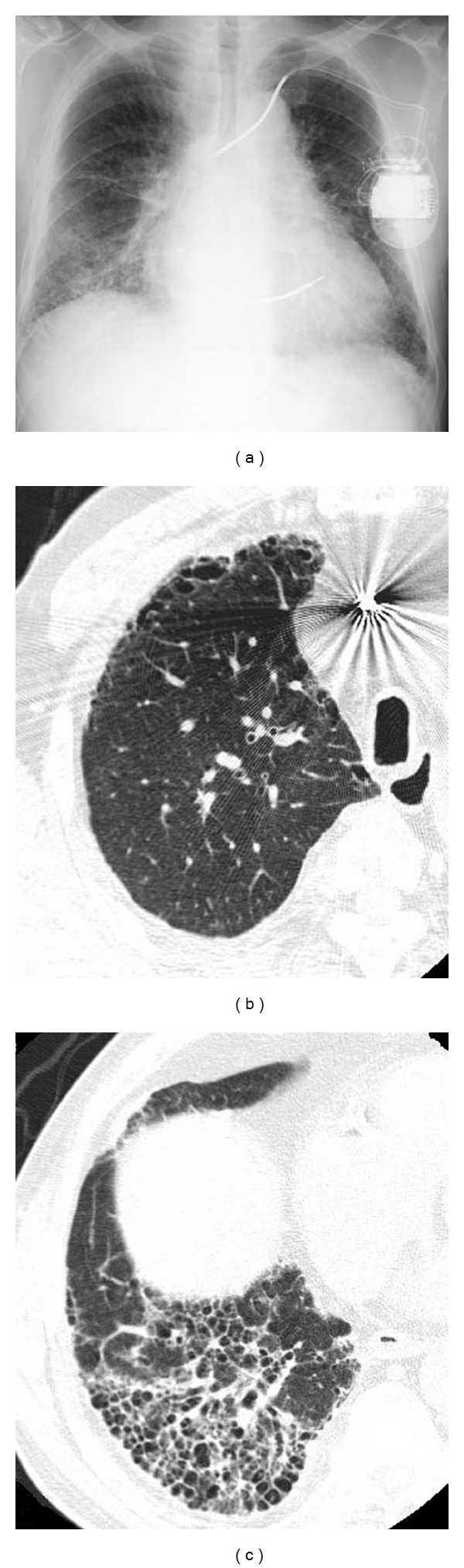
Emphysema with fibrosis, thick-walled large cyst. (a) HRCT of upper lungs shows severe centrilobular emphysema. A relatively thick-walled cyst in the superior basal segment of the left lower lobe. Lung cancer is noted in the lingual division of the left upper lobe. (b) HRCT of left lower lung shows large thick-walled cysts surrounded by ground glass opacity in the regions apart form pleural surface. (c) HRCT of left lower lobe shows multiple bizarre-shaped cysts aggregated in the central portion of the left lower lobe. (d) Pathologic specimens of the resected left upper lobe shows centrilobular cystic lesion involving the membranous and respiratory bronchioles with fibrosis. Note peripheral lung parenchyma spared. (e) Mucus filling in the alveoli with slight septal thickening adjacent to the cyst (circle of Figure 5(e)). Mucus filling and septal thickening correspond to ground glass opacity surrounding large cysts.
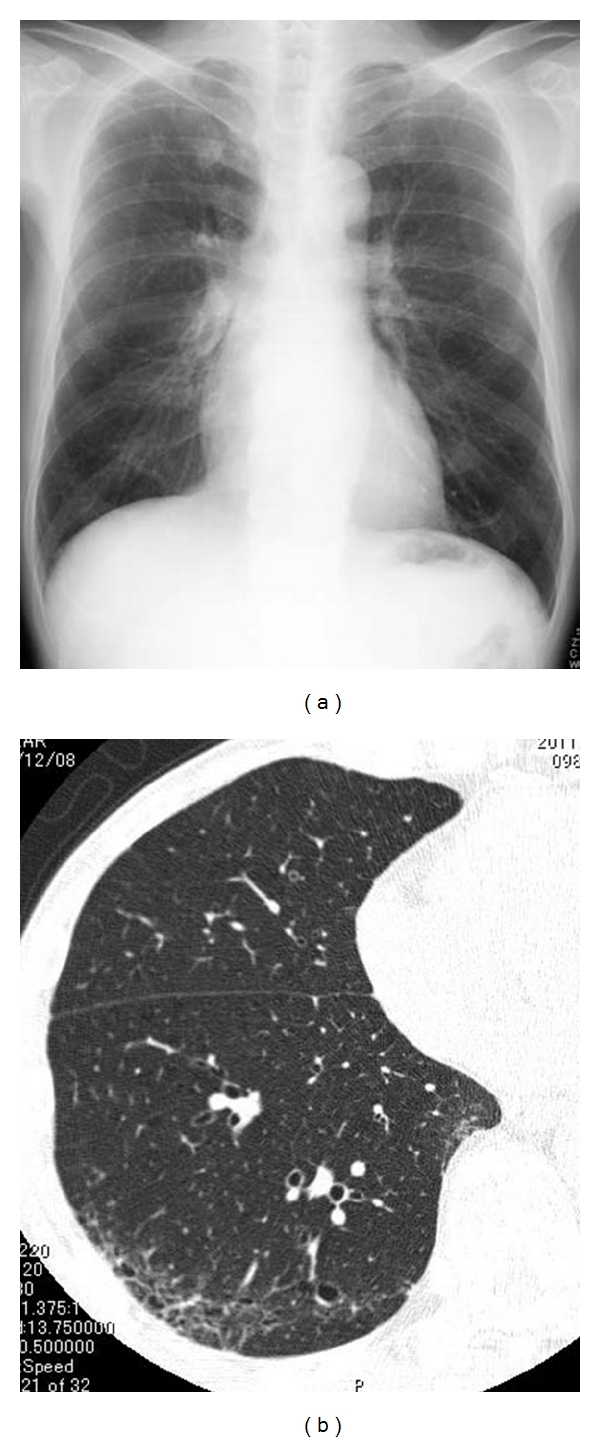
Airway-centered fibrosis with cysts. (a) Chest X-ray shows increased volume of bilateral lungs. (b) High-resolution computed tomography (HRCT) of lower lung shows ground glass opacity and multiple cysts in subpleural region, but these abnormal opacities are predominant in centrilobular region (centrilobular accentuation).
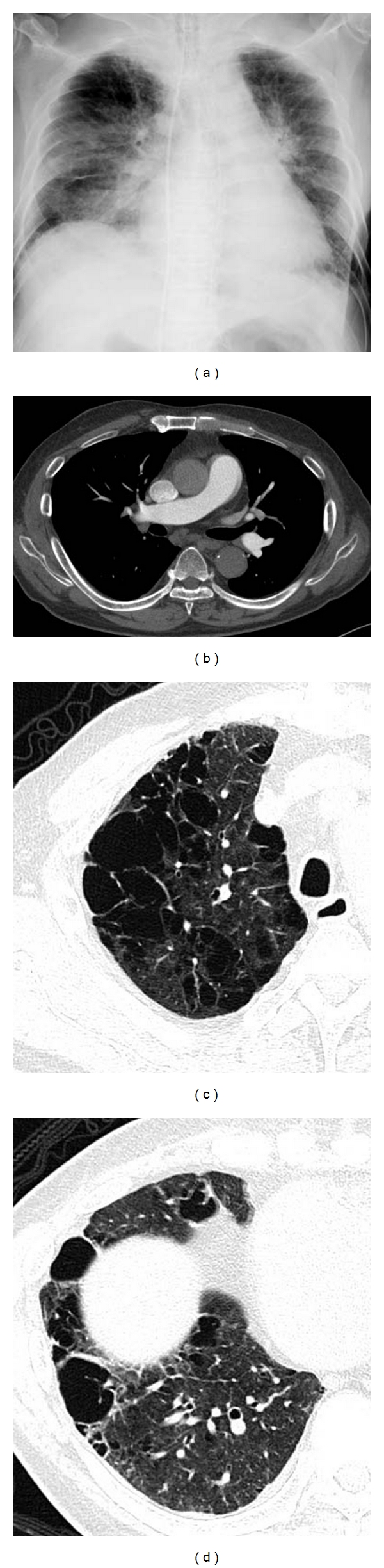
Emphysema with fibrosis, pulmonary hypertension. Estimated right ventricular pressure by cardiac ultrasound is 80 mmHg. (a) Chest X-ray shows cardiomegaly with enlargement of central pulmonary arteries. (b) Contrast-enhanced CT shows dilatation of central pulmonary arteries. There is no evidence of pulmonary thromboembolism. (c) High-resolution computed tomography (HRCT) of upper lung shows severe pulmonary emphysema; some cystic lesions have thick wall. (d) HRCT of the lower lung shows marked destructive change in the lung. There are several large cysts with thick wall.

Emphysema with fibrosis, acute exacerbation by anticancer drug. (a)–(e) Imaging findings before acute exacerbation. (a) Chest X-ray shows normal volume of bilateral lungs. There is reticular opacity in bilateral lower lung fields. (b), (c) High-resolution CT (HRCT). In upper lung, centrilobular emphysema, subpleural cyst, and profuse centrilobular small nodular opacities are identified. In lower lung, subpleural cysts and reticular opacity are noted abutting chest wall, most compatible with UIP pattern. (d)–(f) Imaging findings at acute exacerbation. (d) Chest X-ray shows diffuse ground glass opacity in the left entire lung. Pneumothorax is noted on right side. (e), (f) HRCT shows diffuse ground glass opacity overlapping preexisting interstitial shadow.
Similar articles
-
Combined pulmonary fibrosis and emphysema (CPFE): an entity different from emphysema or pulmonary fibrosis alone.J Thorac Dis. 2015 Apr;7(4):767-79. doi: 10.3978/j.issn.2072-1439.2015.04.17. J Thorac Dis. 2015. PMID: 25973246 Free PMC article. Review.
-
IgG4-related disease presenting with combined pulmonary fibrosis and emphysema (CPFE).Respir Med Case Rep. 2018 Oct 3;25:257-260. doi: 10.1016/j.rmcr.2018.09.017. eCollection 2018. Respir Med Case Rep. 2018. PMID: 30302309 Free PMC article.
-
Heterogeneity in combined pulmonary fibrosis and emphysema.Respiration. 2008;75(4):411-7. doi: 10.1159/000107048. Epub 2007 Aug 6. Respiration. 2008. PMID: 17684315
-
Idiopathic pulmonary fibrosis with emphysema: evidence of synergy among emphysema and idiopathic pulmonary fibrosis in smokers.Respir Care. 2015 Feb;60(2):259-68. doi: 10.4187/respcare.03389. Epub 2014 Nov 11. Respir Care. 2015. PMID: 25389350
-
Effect of combined pulmonary fibrosis and emphysema on patients with connective tissue diseases and systemic sclerosis: a systematic review and meta-analysis.Arthritis Res Ther. 2021 Apr 6;23(1):100. doi: 10.1186/s13075-021-02494-y. Arthritis Res Ther. 2021. PMID: 33823923 Free PMC article.
Cited by
-
Severe pulmonary hypertension due to combined pulmonary fibrosis and emphysema: another cause of death among smokers.Autops Case Rep. 2017 Jun 30;7(2):15-26. doi: 10.4322/acr.2017.022. eCollection 2017 Apr-Jun. Autops Case Rep. 2017. PMID: 28740835 Free PMC article. Review.
-
Quantitative Imaging Methods in Combined Pulmonary Fibrosis and Emphysema.Chest. 2024 Dec;166(6):1463-1472. doi: 10.1016/j.chest.2024.08.007. Epub 2024 Aug 16. Chest. 2024. PMID: 39154797 Free PMC article. Review.
-
The worst of both worlds-combined pulmonary fibrosis and emphysema syndrome.Ann Transl Med. 2016 May;4(10):196. doi: 10.21037/atm.2016.05.26. Ann Transl Med. 2016. PMID: 27294092 Free PMC article. No abstract available.
-
Combined Pulmonary Fibrosis and Emphysema (CPFE) Clinical Features and Management.Int J Chron Obstruct Pulmon Dis. 2021 Jan 28;16:167-177. doi: 10.2147/COPD.S286360. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 33536752 Free PMC article. Review.
-
Radiographic Phenotypes Affect the Risk of Inhaled Corticosteroid-Associated Pneumonia in Patients with COPD.Int J Chron Obstruct Pulmon Dis. 2022 Sep 18;17:2301-2315. doi: 10.2147/COPD.S372735. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 36159655 Free PMC article.
References
-
- Wiggins J, Strickland B, Turner-Warwick M. Combined cryptogenic fibrosing alveolitis and emphysema: the value of high resolution computed tomography in assessment. Respiratory Medicine. 1990;84(5):365–369. - PubMed
-
- Cottin V, Nunes H, Brillet PY, et al. Combined pulmonary fibrosis and emphysema: a distinct underrecognised entity. European Respiratory Journal. 2005;26(4):586–593. - PubMed
-
- Jankowich MD, Polsky M, Klein M, Rounds S. Heterogeneity in combined pulmonary fibrosis and emphysema. Respiration. 2008;75(4):411–417. - PubMed
-
- Nagai S, Hoshino Y, Hayashi M, Ito I. Smoking-related interstitial lung diseases. Current Opinion in Pulmonary Medicine. 2000;6(5):415–419. - PubMed
-
- Ryu JH, Colby TV, Hartman TE, Vassallo R. Smoking-related interstitial lung diseases: a concise review. European Respiratory Journal. 2001;17(1):122–132. - PubMed
LinkOut - more resources
Full Text Sources
