

Bariatric surgery versus intensive medical therapy in obese patients with diabetes
- PMID: 22449319
- PMCID: PMC3372918
- DOI: 10.1056/NEJMoa1200225
Bariatric surgery versus intensive medical therapy in obese patients with diabetes
Abstract
Background: Observational studies have shown improvement in patients with type 2 diabetes mellitus after bariatric surgery.
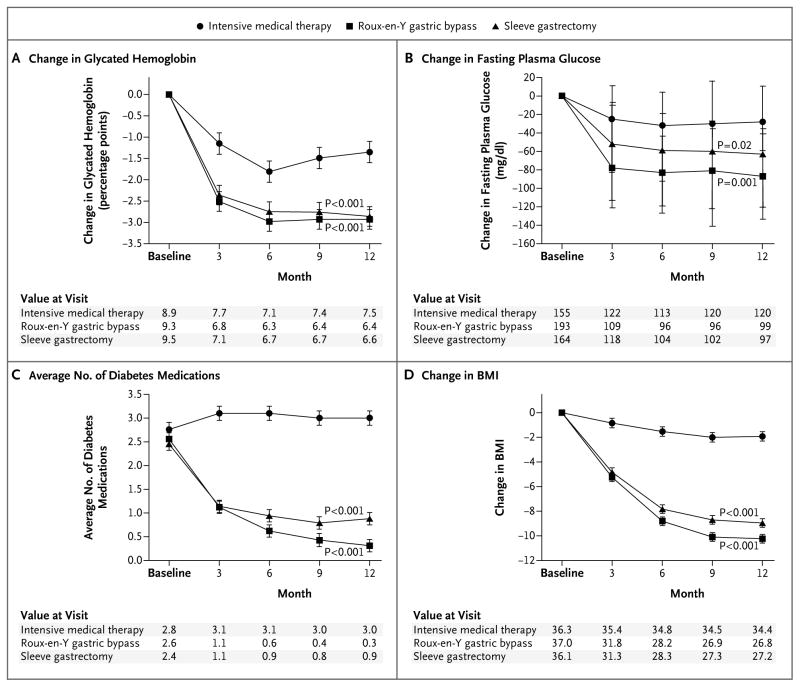
Methods: In this randomized, nonblinded, single-center trial, we evaluated the efficacy of intensive medical therapy alone versus medical therapy plus Roux-en-Y gastric bypass or sleeve gastrectomy in 150 obese patients with uncontrolled type 2 diabetes. The mean (±SD) age of the patients was 49±8 years, and 66% were women. The average glycated hemoglobin level was 9.2±1.5%. The primary end point was the proportion of patients with a glycated hemoglobin level of 6.0% or less 12 months after treatment.
Results: Of the 150 patients, 93% completed 12 months of follow-up. The proportion of patients with the primary end point was 12% (5 of 41 patients) in the medical-therapy group versus 42% (21 of 50 patients) in the gastric-bypass group (P=0.002) and 37% (18 of 49 patients) in the sleeve-gastrectomy group (P=0.008). Glycemic control improved in all three groups, with a mean glycated hemoglobin level of 7.5±1.8% in the medical-therapy group, 6.4±0.9% in the gastric-bypass group (P<0.001), and 6.6±1.0% in the sleeve-gastrectomy group (P=0.003). Weight loss was greater in the gastric-bypass group and sleeve-gastrectomy group (-29.4±9.0 kg and -25.1±8.5 kg, respectively) than in the medical-therapy group (-5.4±8.0 kg) (P<0.001 for both comparisons). The use of drugs to lower glucose, lipid, and blood-pressure levels decreased significantly after both surgical procedures but increased in patients receiving medical therapy only. The index for homeostasis model assessment of insulin resistance (HOMA-IR) improved significantly after bariatric surgery. Four patients underwent reoperation. There were no deaths or life-threatening complications.
Conclusions: In obese patients with uncontrolled type 2 diabetes, 12 months of medical therapy plus bariatric surgery achieved glycemic control in significantly more patients than medical therapy alone. Further study will be necessary to assess the durability of these results. (Funded by Ethicon Endo-Surgery and others; ClinicalTrials.gov number, NCT00432809.).
Figures
Comment in
-
Surgery or medical therapy for obese patients with type 2 diabetes?N Engl J Med. 2012 Apr 26;366(17):1635-6. doi: 10.1056/NEJMe1202443. Epub 2012 Mar 26. N Engl J Med. 2012. PMID: 22449318 No abstract available.
-
Diabetes: On trial--bariatric surgery for treatment of type 2 diabetes mellitus.Nat Rev Endocrinol. 2012 Apr 10;8(6):317. doi: 10.1038/nrendo.2012.57. Nat Rev Endocrinol. 2012. PMID: 22488643 No abstract available.
-
Bariatric surgery or medical therapy for obesity.N Engl J Med. 2012 Aug 2;367(5):473; author reply 474-6. doi: 10.1056/NEJMc1206633. N Engl J Med. 2012. PMID: 22853019 No abstract available.
-
Bariatric surgery or medical therapy for obesity.N Engl J Med. 2012 Aug 2;367(5):473-4; author reply 474-6. doi: 10.1056/NEJMc1206633. N Engl J Med. 2012. PMID: 22853020 No abstract available.
-
Bariatric surgery or medical therapy for obesity.N Engl J Med. 2012 Aug 2;367(5):474; author reply 474-5. doi: 10.1056/NEJMc1206633. N Engl J Med. 2012. PMID: 22853021 No abstract available.
-
Bariatric intervention effective at reversing Type 2 diabetes.Evid Based Med. 2013 Apr;18(2):68-9. doi: 10.1136/eb-2012-100834. Epub 2012 Aug 25. Evid Based Med. 2013. PMID: 22923707 No abstract available.
-
Bariatric surgery or medicine for type 2 diabetes?Expert Opin Pharmacother. 2012 Oct;13(15):2249-53. doi: 10.1517/14656566.2012.721779. Epub 2012 Sep 8. Expert Opin Pharmacother. 2012. PMID: 22957791
-
The surgical cure for diabetes?Natl Med J India. 2012 Sep-Oct;25(5):281-3. Natl Med J India. 2012. PMID: 23448628 No abstract available.
-
[Bariatric surgery and diabetes mellitus: pioneering studies from 2012 and consequences for treatment strategies].Internist (Berl). 2013 May;54(5):639-44. doi: 10.1007/s00108-013-3274-z. Internist (Berl). 2013. PMID: 23568061 German. No abstract available.
-
Update in general internal medicine: evidence published in 2012.Ann Intern Med. 2013 Apr 16;158(8):615-9. doi: 10.7326/0003-4819-158-8-201304160-00101. Ann Intern Med. 2013. PMID: 23579948 No abstract available.
-
Update in endocrinology: evidence published in 2012.Ann Intern Med. 2013 Jun 4;158(11):821-4. doi: 10.7326/0003-4819-158-11-201306040-00106. Ann Intern Med. 2013. PMID: 23580066 No abstract available.
References
-
- Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2. 7 million participants. Lancet. 2011;378:31–40. - PubMed
-
- Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193–203. - PMC - PubMed
-
- Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA. 2004;291:335–42. - PubMed
-
- Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:3, 248.e5–256.e5. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials