

Recent advances in acute kidney injury epidemiology
- PMID: 22449946
- PMCID: PMC3357067
- DOI: 10.1097/MNH.0b013e3283521d95
Recent advances in acute kidney injury epidemiology
Abstract
Purpose of review: Expanding rates of acute kidney injury (AKI) coupled with increasing awareness of its short-term and long-term sequelae have focused efforts to identify patients at risk for this disease and its complications. This review details the recent attempts to identify novel risk factors for AKI, describes further refinements in the diagnostic and prognostic approach using biological markers of injury, and highlights the features of AKI that independently predict poor long-term outcomes.
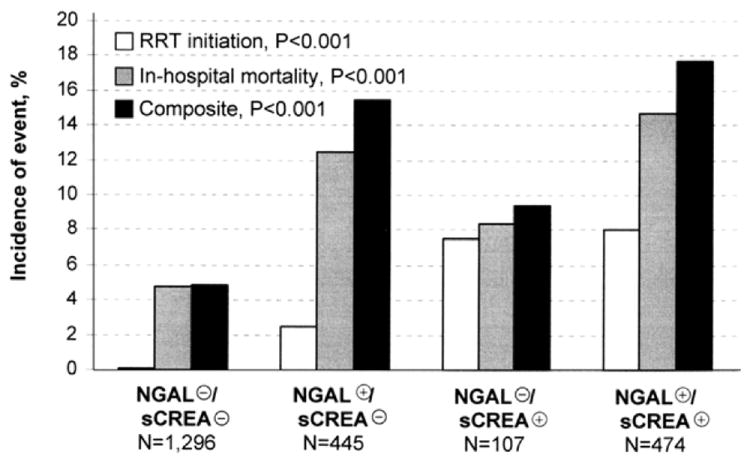
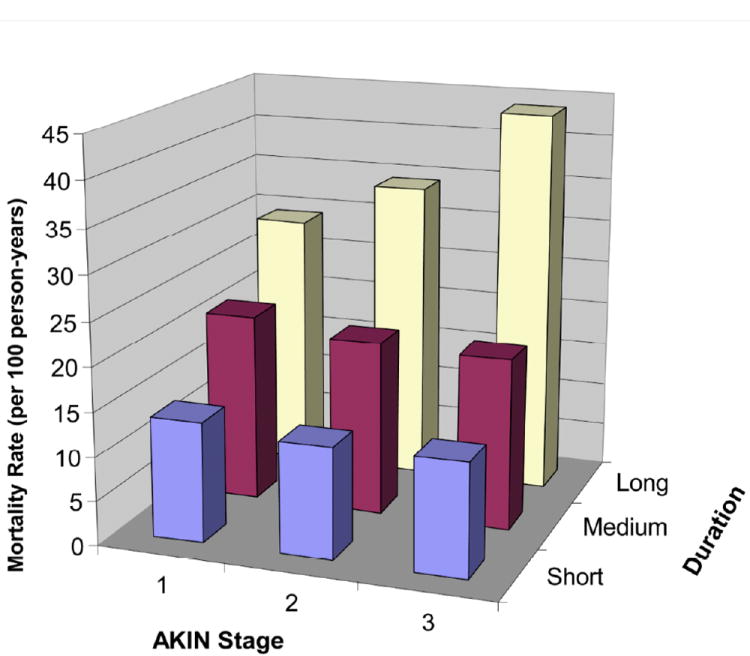
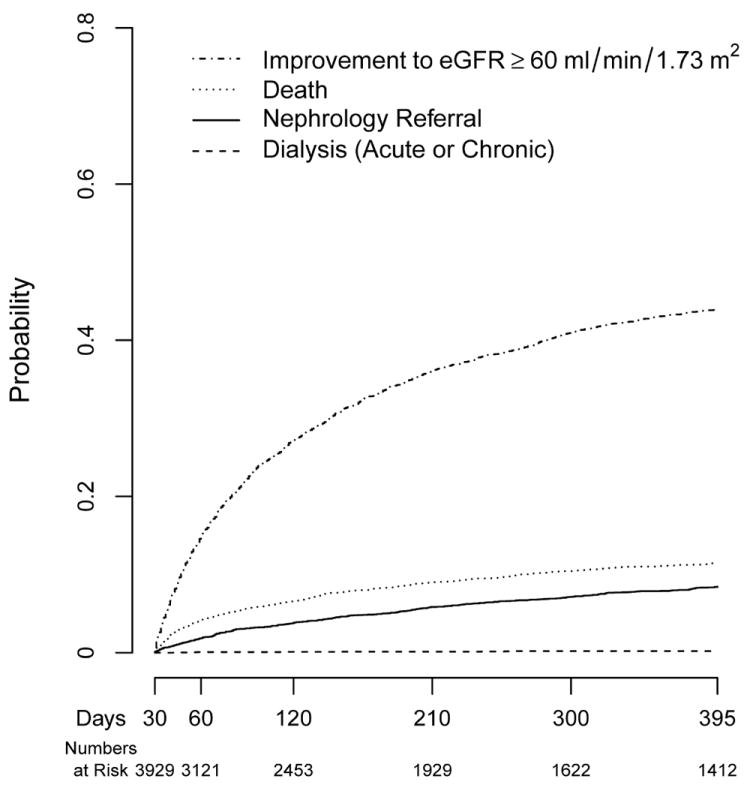
Recent findings: The presence of proteinuria predicts the development of AKI independently of estimated glomerular filtration rate. Initial results from a large prospective study of AKI biomarkers in cardiac surgery indicate lower agreement with serum creatinine as an AKI standard than observed in early studies. AKI severity and duration are important predictors of chronic kidney disease and long-term mortality. A minority of patients surviving AKI with decreased kidney function is seen by a nephrologist.
Summary: Although the pathophysiologic link is unclear, proteinuria is an easily measurable risk factor for AKI worth considering before anticipated procedures or medication exposures carrying nephrologic risk. Investigation extending beyond agreement with serum creatinine is needed to fully understand the diagnostic and prognostic value of AKI biomarkers. Severity and duration are components of AKI that can help risk-stratify survivors in need of monitoring or nephrology referral.
Conflict of interest statement
Conflict of Interest: EDS has a consulting arrangement with Alere, Inc.
Figures
References
-
- Xue JL, Daniels F, Star RA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol. 2006;17:1135–1142. - PubMed
-
- Mehta RL, Pascual MT, Soroko S, et al. Spectrum of acute renal failure in the intensive care unit: the PICARD experience. Kidney Int. 2004;66:1613–1621. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. Jama. 2005;294:813–818. - PubMed
-
- Chertow GM, Burdick E, Honour M, et al. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365–3370. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
