

Eosinophilic esophagitis: diagnostic tests and criteria
- PMID: 22450900
- PMCID: PMC4591255
- DOI: 10.1097/MOG.0b013e328352b5ef
Eosinophilic esophagitis: diagnostic tests and criteria
Abstract
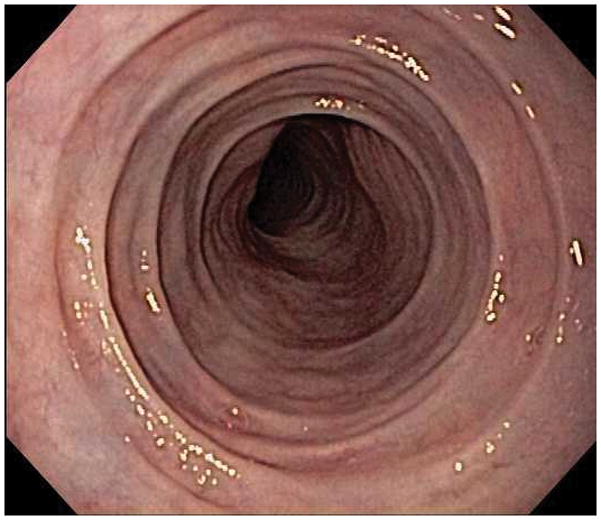
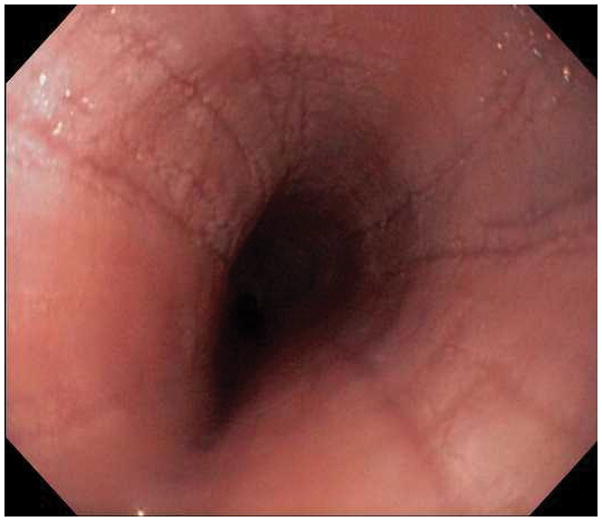
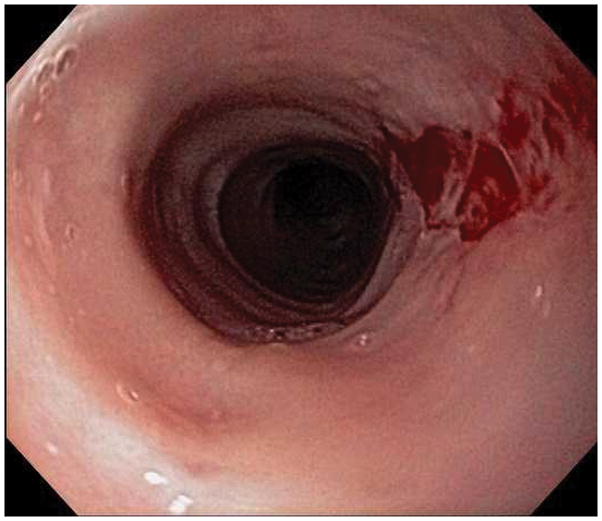
Purpose of review: To present the clinical, endoscopic, and histologic features of eosinophilic esophagitis (EoE), review the current diagnostic guidelines for EoE, and present an approach for diagnosis of EoE. It will also highlight selected techniques that are under development that may be useful in the future for diagnosis of EoE.
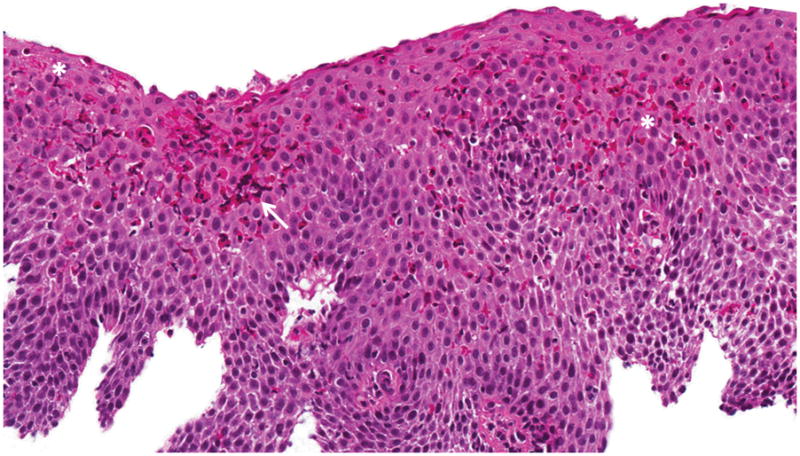
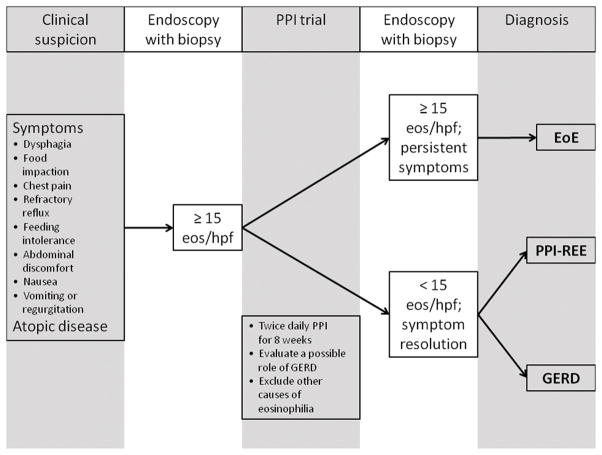
Recent findings: Recently updated guidelines emphasize that EoE is a clinicopathologic condition. Specifically, three criteria must be met to diagnose EoE: clinical symptoms of esophageal dysfunction; an esophageal biopsy with a maximum eosinophil count of at least 15 eosinophils per high-power microscopy field, with few exceptions; and exclusion of other possible causes of esophageal eosinophilia, including proton-pump inhibitor responsive esophageal eosinophilia (PPI-REE). A PPI trial is typically required both to assess for PPI-REE and to evaluate for the presence of concomitant gastroesophageal reflux disease.
Summary: EoE is a chronic, immune-mediated disorder. Because no single symptom, endoscopic finding, or histopathologic feature is pathognomonic, diagnosis can be challenging. In the future, symptom scores, tissue or serum biomarkers, and genetic testing may play a role in diagnosis, but these methods have yet to be validated and are not yet recommended for routine clinical use.
Conflict of interest statement
The author has no conflicts pertaining to this manuscript.
Figures


Similar articles
-
Markers of eosinophilic inflammation for diagnosis of eosinophilic esophagitis and proton pump inhibitor-responsive esophageal eosinophilia: a prospective study.Clin Gastroenterol Hepatol. 2014 Dec;12(12):2015-22. doi: 10.1016/j.cgh.2014.06.019. Epub 2014 Jun 30. Clin Gastroenterol Hepatol. 2014. PMID: 24993367 Free PMC article.
-
Diagnosis and treatment of eosinophilic esophagitis in clinical practice.Clin J Gastroenterol. 2017 Apr;10(2):87-102. doi: 10.1007/s12328-017-0725-4. Epub 2017 Feb 28. Clin J Gastroenterol. 2017. PMID: 28247277 Review.
-
Diagnostics of eosinophilic esophagitis: clinical, endoscopic, and histologic pitfalls.Dig Dis. 2014;32(1-2):48-53. doi: 10.1159/000357009. Epub 2014 Feb 28. Dig Dis. 2014. PMID: 24603380 Free PMC article. Review.
-
Diagnosis of eosinophilic esophagitis: current approach and future directions.Curr Gastroenterol Rep. 2011 Jun;13(3):240-6. doi: 10.1007/s11894-011-0183-y. Curr Gastroenterol Rep. 2011. PMID: 21360070 Review.
-
[Proton Pump Inhibitor-responsive Esophageal Eosinophilia: An Overview of Cases from One University Hospital Center].Korean J Gastroenterol. 2016 Apr 25;67(4):178-82. doi: 10.4166/kjg.2016.67.4.178. Korean J Gastroenterol. 2016. PMID: 27112243 Korean.
Cited by
-
Epidemiology and the Growing Epidemic of Food Allergy in Children and Adults Across the Globe.Curr Allergy Asthma Rep. 2024 Mar;24(3):95-106. doi: 10.1007/s11882-023-01120-y. Epub 2024 Jan 12. Curr Allergy Asthma Rep. 2024. PMID: 38214821 Review.
-
Biological data annotation via a human-augmenting AI-based labeling system.NPJ Digit Med. 2021 Oct 7;4(1):145. doi: 10.1038/s41746-021-00520-6. NPJ Digit Med. 2021. PMID: 34620993 Free PMC article.
-
A Deep Multi-Label Segmentation Network For Eosinophilic Esophagitis Whole Slide Biopsy Diagnostics.Annu Int Conf IEEE Eng Med Biol Soc. 2022 Jul;2022:3211-3217. doi: 10.1109/EMBC48229.2022.9871086. Annu Int Conf IEEE Eng Med Biol Soc. 2022. PMID: 36085661 Free PMC article.
-
Esophageal lichen planus: Current knowledge, challenges and future perspectives.World J Gastroenterol. 2022 Nov 7;28(41):5893-5909. doi: 10.3748/wjg.v28.i41.5893. World J Gastroenterol. 2022. PMID: 36405107 Free PMC article. Review.
-
Eosinophilic Gastrointestinal Diseases: The Pathogenesis, Diagnosis, and Treatment.Intern Med. 2023 Jan 1;62(1):1-10. doi: 10.2169/internalmedicine.8417-21. Epub 2021 Oct 19. Intern Med. 2023. PMID: 34670903 Free PMC article.
References
-
- Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20. e6. This is the recently published updated consensus guidelines for diagnosis and treatmnt of EoE. This presents the currently accepted diagnostic criteria for EoE, and also is an excellent review of the most recent evidence base in the field. - PubMed
-
- Landres RT, Kuster GG, Strum WB. Eosinophilic esophagitis in a patient with vigorous achalasia. Gastroenterology. 1978;74:1298–1301. - PubMed
-
- Attwood SE, Smyrk TC, Demeester TR, et al. Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome. Dig Dis Sci. 1993;38:109–16. - PubMed
-
- Noel RJ, Putnam PE, Rothenberg ME. Eosinophilic esophagitis. N Engl J Med. 2004;351:940–1. - PubMed
-
- Hruz P, Straumann A, Bussmann C, et al. Escalating incidence of eosinophilic esophagitis: A 20-year prospective, population-based study in Olten County, Switzerland. J Allergy Clin Immunol. 2011;128:1349–1350. e5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
