

Progression in smoldering Waldenstrom macroglobulinemia: long-term results
- PMID: 22451426
- PMCID: PMC3362362
- DOI: 10.1182/blood-2011-10-384768
Progression in smoldering Waldenstrom macroglobulinemia: long-term results
Abstract
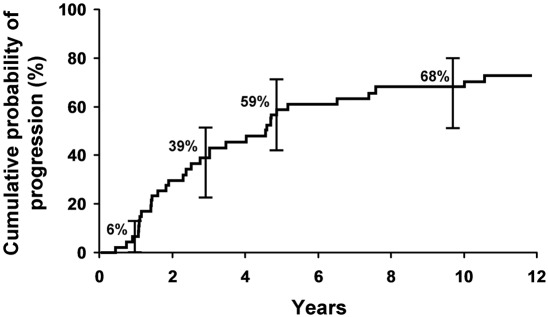
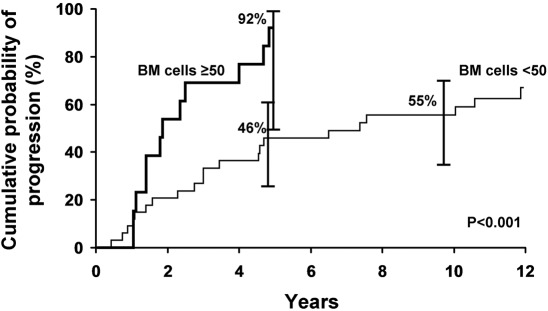
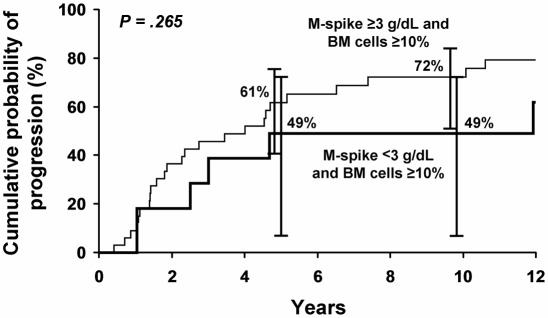
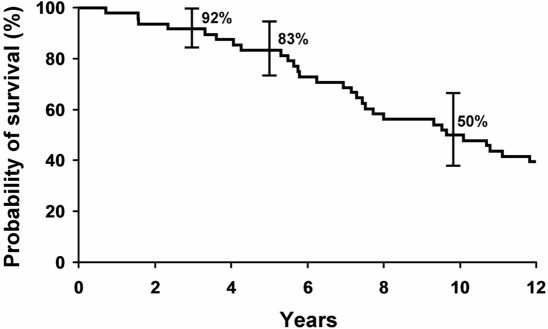
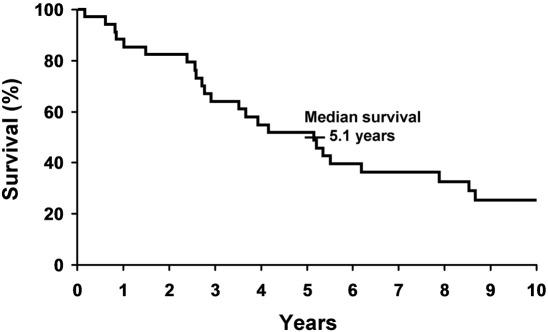
The purpose of this study was to define the risk of progression and survival of patients with smoldering Waldenström macroglobulinemia (SWM). SWM is defined clinically as having a serum monoclonal IgM protein≥3 g/dL and/or≥10% bone marrow lymphoplasmacytic infiltration but no evidence of end-organ damage (anemia, constitutional symptoms, hyperviscosity, lymphadenopathy, or hepatosplenomegaly). We searched a computerized database and reviewed the medical records of all patients at Mayo Clinic who fulfilled the criteria of SWM between 1974 and 1995. During 285 cumulative person-years of follow-up of the 48 patients with SWM (median, 15.4 years), 34 (71%) progressed to symptomatic Waldenström macroglobulinemia (WM) requiring treatment, one to primary amyloidosis, and one to lymphoma (total, 75%). The cumulative probability of progression to symptomatic WM, amyloidosis, or lymphoma was 6% at 1 year, 39% at 3 years, 59% at 5 years, and 68% at 10 years. The major risk factors for progression were percentage of lymphoplasmacytic cells in the bone marrow, size of the serum M-spike, and the hemoglobin value. Patients with SWM should be followed and not treated until symptomatic WM develops. Treatment on a clinical trial for those at greatest risk of progression should be considered.
Figures
References
-
- Waldenstrom J. Incipient myelomatosis or “essential” hyperglobulinemia with fibrinogenopenia: a new syndrome? Acta Med Scand. 1944;117:216–247.
-
- Owen RG, Treon SP, Al-Katib A, et al. Clinicopathological definition of Waldenstrom's macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom's Macroglobulinemia. Semin Oncol. 2003;30(2):110–115. - PubMed
-
- Kyle RA, Treon SP, Alexanian R, et al. Prognostic markers and criteria to initiate therapy in Waldenstrom's macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom's Macroglobulinemia [review]. Semin Oncol. 2003;30(2):116–120. - PubMed
-
- Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–481.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
