

Effectiveness of physical activity promotion based in primary care: systematic review and meta-analysis of randomised controlled trials
- PMID: 22451477
- PMCID: PMC3312793
- DOI: 10.1136/bmj.e1389
Effectiveness of physical activity promotion based in primary care: systematic review and meta-analysis of randomised controlled trials
Abstract
Objectives: To determine whether trials of physical activity promotion based in primary care show sustained effects on physical activity or fitness in sedentary adults, and whether exercise referral interventions are more effective than other interventions.
Design: Systematic review and meta-analysis of randomised controlled trials.
Data sources: Medline, CINAHL, PsycINFO, EMBASE, SPORTDiscus, Centre for Reviews and Dissemination, the Cochrane Library, and article reference lists.
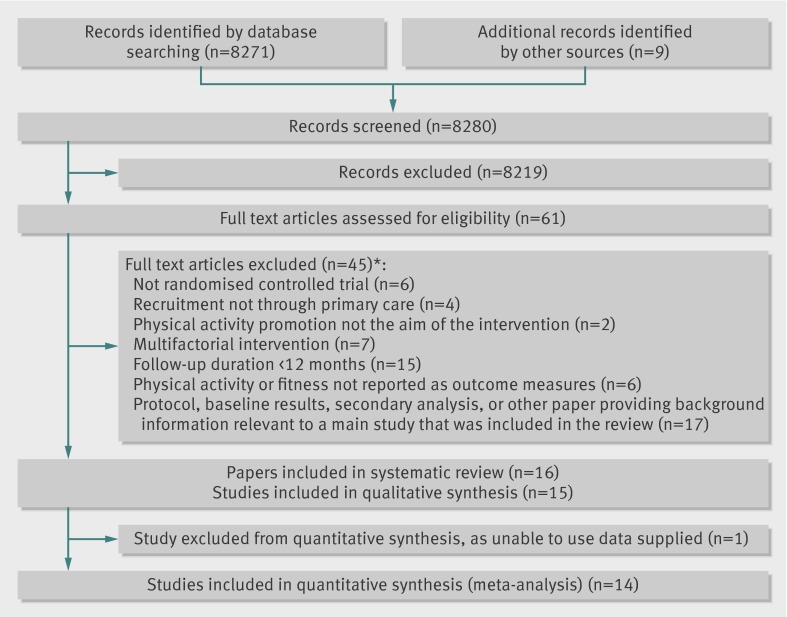
Review methods: Review of randomised controlled trials of physical activity promotion in sedentary adults recruited in primary care, with minimum follow-up of 12 months, reporting physical activity or fitness (or both) as outcomes, and using intention to treat analyses. Two reviewers independently assessed studies for inclusion, appraised risk of bias, and extracted data. Pooled effect sizes were calculated using a random effects model.
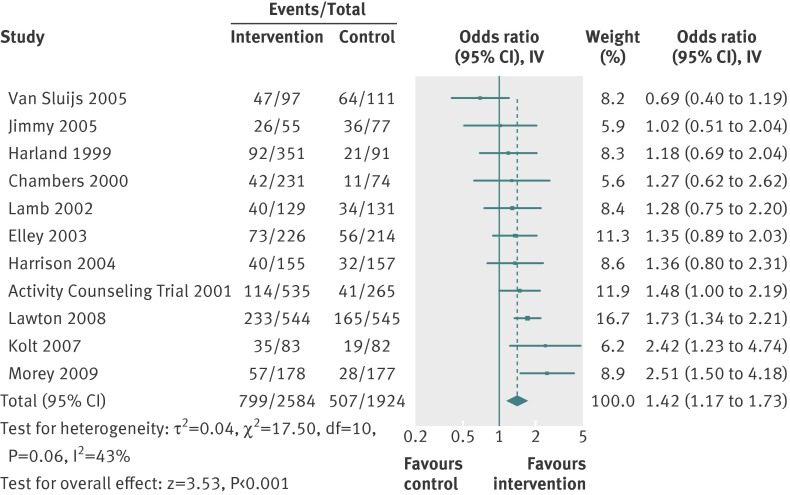
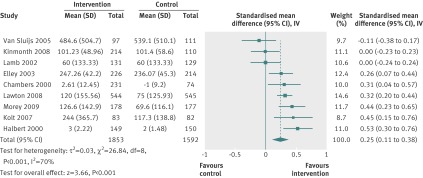
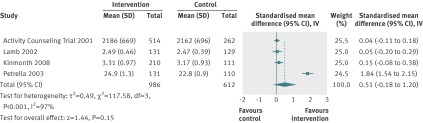
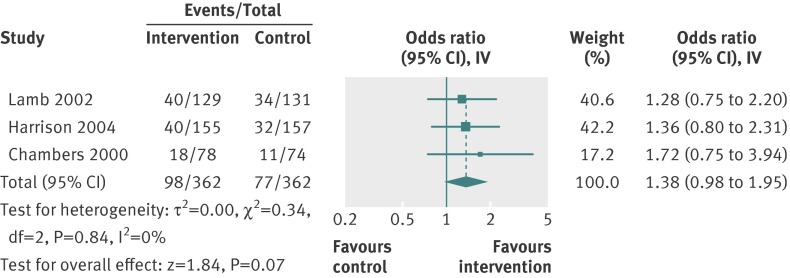
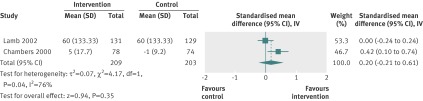
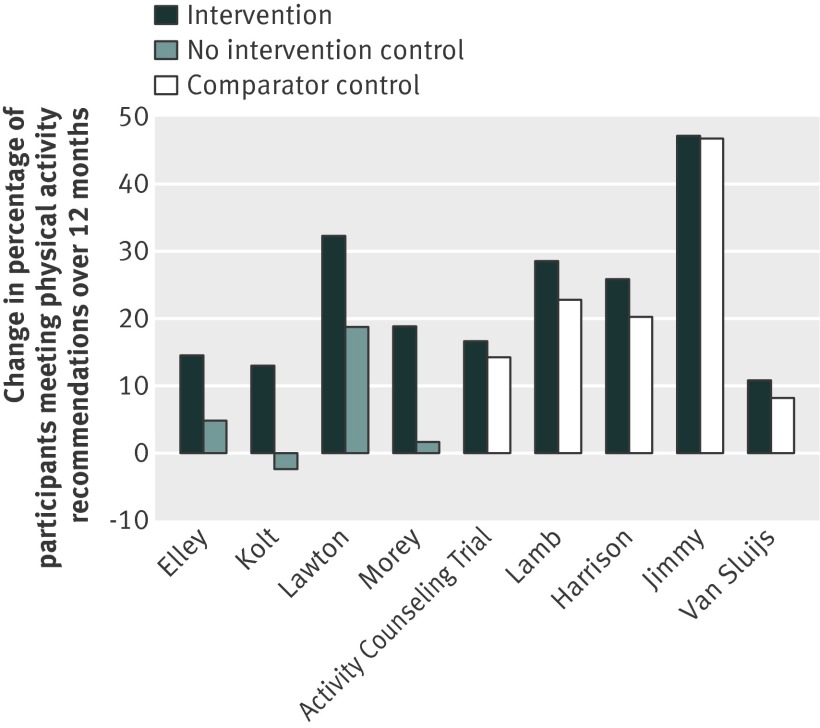
Results: We included 15 trials (n=8745). Most interventions took place in primary care, included health professionals in delivery, and involved advice or counselling given face to face or by phone (or both) on multiple occasions. Only three trials investigated exercise referral. In 13 trials presenting self reported physical activity, we saw small to medium positive intervention effects at 12 months (odds ratio 1.42, 95% confidence interval 1.17 to 1.73; standardised mean difference 0.25, 0.11 to 0.38). The number needed to treat with an intervention for one additional sedentary adult to meet internationally recommended levels of activity at 12 months was 12 (7 to 33). In four trials reporting cardiorespiratory fitness, a medium positive effect at 12 months was non-significant (standardised mean difference 0.51, -0.18 to 1.20). Three trials of exercise referral found small non-significant effects on self reported physical activity at 12 months (odds ratio 1.38; 0.98 to 1.95; standardised mean difference 0.20, -0.21 to 0.61).
Conclusions: Promotion of physical activity to sedentary adults recruited in primary care significantly increases physical activity levels at 12 months, as measured by self report. We found insufficient evidence to recommend exercise referral schemes over advice or counselling interventions. Primary care commissioners should consider these findings while awaiting further trial evaluation of exercise referral schemes and other primary care interventions, with longer follow-up and use of objective measures of outcome.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Republished in
-
Republished research: effectiveness of physical activity promotion based in primary care: systematic review and meta-analysis of randomised controlled trials.Br J Sports Med. 2013 Jan;47(1):27. doi: 10.1136/bjsports-2012-e1389rep. Br J Sports Med. 2013. PMID: 23243114
Comment in
-
Brief health professional-provided interventions may lead to small improvements in physical activity.Evid Based Med. 2013 Feb;18(1):e1. doi: 10.1136/ebmed-2012-100761. Epub 2012 Jun 20. Evid Based Med. 2013. PMID: 22718985 No abstract available.
-
Physical activity promotion in primary care has a sustained influence on activity levels of sedentary adults.Br J Sports Med. 2014 Jul;48(13):1069-70. doi: 10.1136/bjsports-2013-093187. Epub 2013 Nov 20. Br J Sports Med. 2014. PMID: 24258533 No abstract available.
References
-
- Chief medical officers of England, Scotland, Wales and Northern Island. Start active, stay active: a report on physical activity from the four home countries’ chief medical officers. Department of Health, 2011.
-
- Woodcock J, Franco OH, Orsini N, Roberts I. Non-vigorous physical activity and all-cause mortality: systematic review and meta-analysis of cohort studies. Int J Epidemiol 2011;40:121-38. - PubMed
-
- Joint Health Surveys Unit. Health survey for England 2008. Physical activity and fitness. The Stationery Office, 2009.
-
- Craig A, Dinan S, Smith A, Taylor A, Webborn N. The National Quality Assurance Framework for Exercise Referral Systems. Department of Health, 2001.
-
- Williams NH. “The wise, for cure, on exercise depend”: physical activity interventions in primary care in Wales. Br J Sports Med 2009;43:106-8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical