

Rhombencephalosynapsis: a hindbrain malformation associated with incomplete separation of midbrain and forebrain, hydrocephalus and a broad spectrum of severity
- PMID: 22451504
- PMCID: PMC3338925
- DOI: 10.1093/brain/aws065
Rhombencephalosynapsis: a hindbrain malformation associated with incomplete separation of midbrain and forebrain, hydrocephalus and a broad spectrum of severity
Abstract
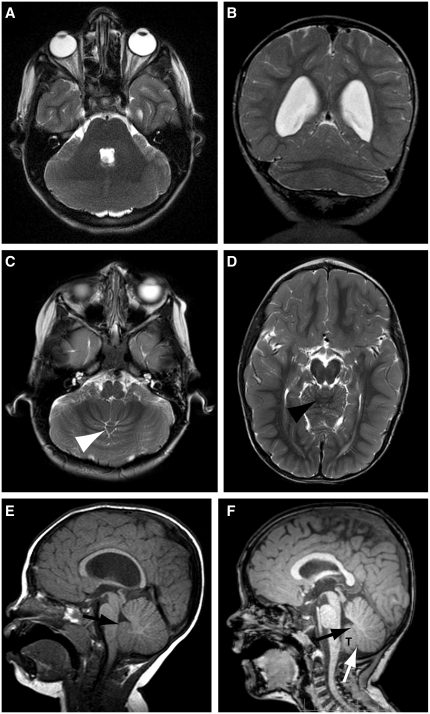
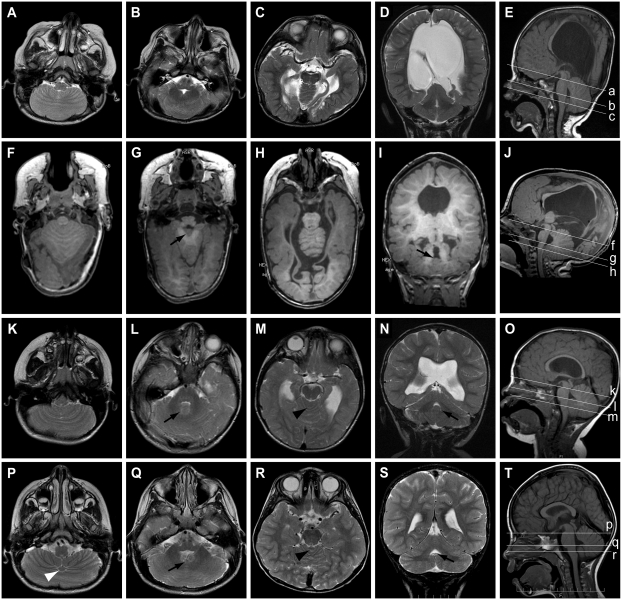
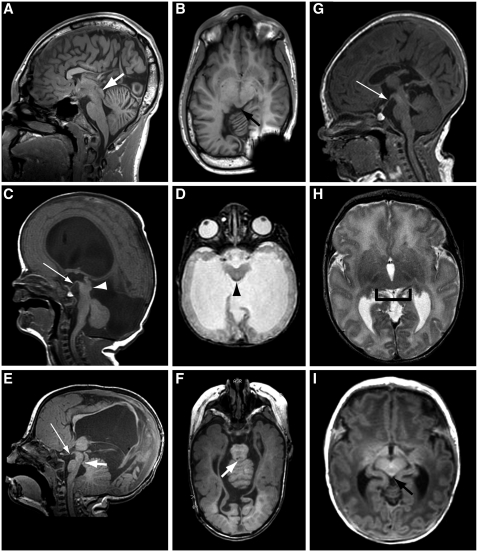
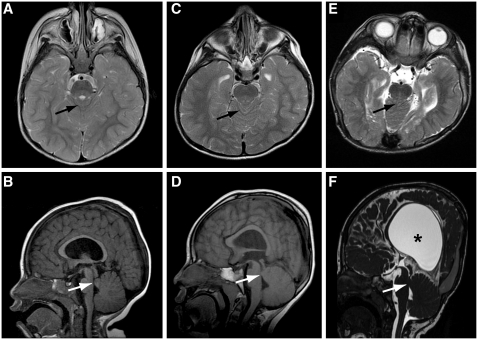
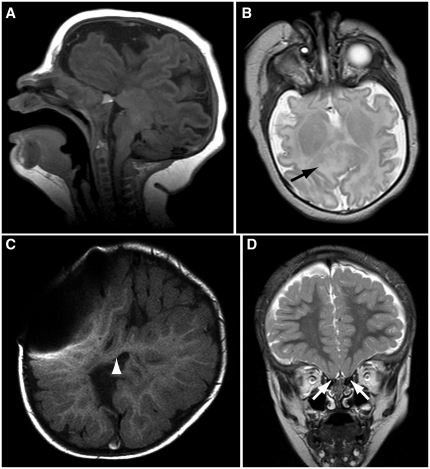
Rhombencephalosynapsis is a midline brain malformation characterized by missing cerebellar vermis with apparent fusion of the cerebellar hemispheres. Rhombencephalosynapsis can be seen in isolation or together with other central nervous system and extra-central nervous system malformations. Gómez-López-Hernández syndrome combines rhombencephalosynapsis with parietal/temporal alopecia and sometimes trigeminal anaesthesia, towering skull shape and dysmorphic features. Rhombencephalosynapsis can also be seen in patients with features of vertebral anomalies, anal atresia, cardiovascular anomalies, trachea-oesophageal fistula, renal anomalies, limb defects (VACTERL) association. Based on a comprehensive evaluation of neuroimaging findings in 42 patients with rhombencephalosynapsis, we propose a spectrum of severity, ranging from mild (the partial absence of nodulus, anterior and posterior vermis), to moderate (the absence of posterior vermis with some anterior vermis and nodulus present), to severe (the absence of posterior and anterior vermis with some nodulus present), to complete (the absence of the entire vermis including nodulus). We demonstrate that the severity of rhombencephalosynapsis correlates with fusion of the tonsils, as well as midbrain abnormalities including aqueductal stenosis and midline fusion of the tectum. Rhombencephalosynapsis is also associated with multiple forebrain abnormalities including absent olfactory bulbs, dysgenesis of the corpus callosum, absent septum pellucidum and, in rare patients, atypical forms of holoprosencephaly. The frequent association between rhombencephalosynapsis and aqueductal stenosis prompted us to evaluate brain magnetic resonance images in other patients with aqueductal stenosis at our institution, and remarkably, we identified rhombencephalosynapsis in 9%. Strikingly, subjects with more severe rhombencephalosynapsis have more severely abnormal neurodevelopmental outcome, as do subjects with holoprosencephaly and patients with VACTERL features. In summary, our data provide improved diagnostic and prognostic information, and support disruption of dorsal-ventral patterning as a mechanism underlying rhombencephalosynapsis.
Figures
Comment in
-
Rhombencephalosynapsis: new findings in a larger study.Brain. 2012 May;135(Pt 5):1346-7. doi: 10.1093/brain/aws089. Epub 2012 Apr 4. Brain. 2012. PMID: 22492564 No abstract available.
Similar articles
-
Rhombencephalosynapsis: new findings in a larger study.Brain. 2012 May;135(Pt 5):1346-7. doi: 10.1093/brain/aws089. Epub 2012 Apr 4. Brain. 2012. PMID: 22492564 No abstract available.
-
Rhomboencephalosynapsis: Review of the Literature.World Neurosurg. 2022 Mar;159:48-53. doi: 10.1016/j.wneu.2021.12.062. Epub 2021 Dec 22. World Neurosurg. 2022. PMID: 34954057 Review.
-
Beyond Gómez-López-Hernández syndrome: recurring phenotypic themes in rhombencephalosynapsis.Am J Med Genet A. 2012 Oct;158A(10):2393-406. doi: 10.1002/ajmg.a.35561. Epub 2012 Sep 10. Am J Med Genet A. 2012. PMID: 22965664 Free PMC article.
-
Rhombencephalosynapsis as a cause of aqueductal stenosis: an under-recognized association in hydrocephalic children.Pediatr Radiol. 2014 Jul;44(7):849-56. doi: 10.1007/s00247-014-2877-4. Epub 2014 Mar 16. Pediatr Radiol. 2014. PMID: 24633306
-
Genetic evaluation including exome sequencing of two patients with Gomez-Lopez-Hernandez syndrome: Case reports and review of the literature.Am J Med Genet A. 2020 Apr;182(4):623-627. doi: 10.1002/ajmg.a.61496. Epub 2020 Jan 31. Am J Med Genet A. 2020. PMID: 32003537 Review.
Cited by
-
Midbrain and hindbrain malformations: advances in clinical diagnosis, imaging, and genetics.Lancet Neurol. 2013 Apr;12(4):381-93. doi: 10.1016/S1474-4422(13)70024-3. Epub 2013 Mar 18. Lancet Neurol. 2013. PMID: 23518331 Free PMC article. Review.
-
Rhombencephalosynapsis: a rare congenital malformation.Acta Neurol Belg. 2023 Oct;123(5):2021-2022. doi: 10.1007/s13760-022-02080-2. Epub 2022 Sep 6. Acta Neurol Belg. 2023. PMID: 36064837 No abstract available.
-
Expanding the spectrum of congenital anomalies of the diencephalic-mesencephalic junction.Neuroradiology. 2016 Jan;58(1):33-44. doi: 10.1007/s00234-015-1601-x. Epub 2015 Oct 7. Neuroradiology. 2016. PMID: 26446148
-
Neuropsychiatric Symptoms in Rhombencephalosynapsis: A Clinical Report.Cerebellum. 2024 Dec;23(6):2671-2678. doi: 10.1007/s12311-024-01740-8. Epub 2024 Sep 4. Cerebellum. 2024. PMID: 39230845 Free PMC article.
-
Rhombencephalosynapsis: A Rare Hindbrain Malformation.Cureus. 2024 Jul 26;16(7):e65400. doi: 10.7759/cureus.65400. eCollection 2024 Jul. Cureus. 2024. PMID: 39184610 Free PMC article.
References
-
- Adam MP, Abramowsky CR, Brady AN, Coleman K, Todd NW. Rhabdomyomatous hamartomata of the pharyngeal region with bilateral microtia and aural atresia: a new association? Birth Defects Res Part A, Clin Mol Teratol. 2007;79:242–8. - PubMed
-
- Alkan O, Kizilkilic O, Yildirim T. Malformations of the midbrain and hindbrain: a retrospective study and review of the literature. Cerebellum. 2009;8:355–65. - PubMed
-
- Barth PG. Rhombencephalosynapsis In: Harvey BS, Paolo C, editors. . Handbook of clinical neurology, Vol 87 (3rd series) malformations of the nervous system. Amsterdam: Elsevier BV; 2008. p. 53–65. - PubMed
-
- Boltenstern M, Konrad A, Jost W, Uder M, Kujat C. [Rhombencephalosynapsis] RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin. 1995;163:91–3. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
