

Endoscopy-assisted iliotibial tract harvesting for skull base reconstruction: feasibility on a cadaveric model
- PMID: 22451823
- PMCID: PMC3312104
- DOI: 10.1055/s-0031-1275260
Endoscopy-assisted iliotibial tract harvesting for skull base reconstruction: feasibility on a cadaveric model
Abstract
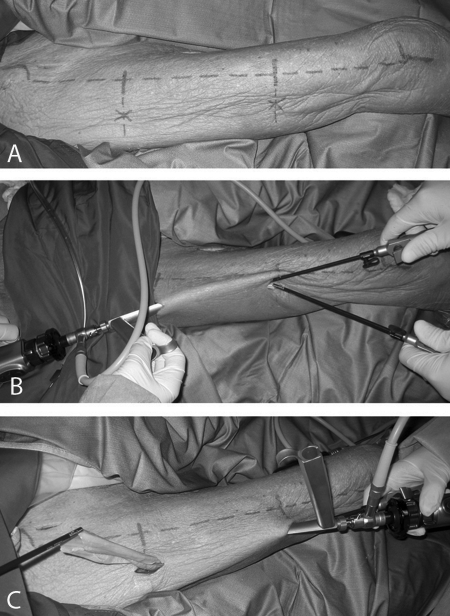
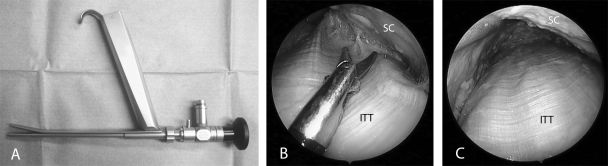
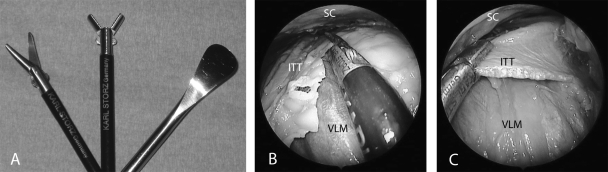
During the last years, multiple methods and a wide set of materials for skull base reconstruction have been described. In our experience, the ideal graft for duraplasty is the iliotibial tract due to its favorable characteristics in terms of thickness, pliability, and strength. In this report, we show the iliotibial tract-harvesting technique under endoscopic guidance with a minimally invasive approach using a cadaveric model. Two longitudinal incisions of 1 cm each were made at 4 cm down a line drawn between the anterior-superior iliac spine and the lateral margin of patella at the extremities of the middle third of the thigh. By using a set of instruments for endoscopic face-lifting, the graft was easily set up and harvested. The endoscopic approach is associated with less visible scars, but longer operative time in comparison with open traditional procedure. The pros and cons in terms of morbidity need to be evaluated by further studies on actual cases.
Keywords: Iliotibial tract; cadaveric model; endoscopic harvesting; skull base reconstruction.
Figures
References
-
- Prevedello D M, Barges-Coll J, Fernandez-Miranda J C, et al. Middle turbinate flap for skull base reconstruction: cadaveric feasibility study. Laryngoscope. 2009;119:2094–2098. - PubMed
-
- Fortes F SG, Carrau R L, Snyderman C H, et al. The posterior pedicle inferior turbinate flap: a new vascularized flap for skull base reconstruction. Laryngoscope. 2007;117:1329–1332. - PubMed
-
- Shah R N, Surowitz J B, Patel M R, et al. Endoscopic pedicled nasoseptal flap reconstruction for pediatric skull base defects. Laryngoscope. 2009;119:1067–1075. - PubMed
-
- Tabaee A, Anand V K, Brown S M, Lin J W, Schwartz T H. Algorithm for reconstruction after endoscopic pituitary and skull base surgery. Laryngoscope. 2007;117:1133–1137. - PubMed
-
- Hadad G, Bassagasteguy L, Carrau R L, et al. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope. 2006;116:1882–1886. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
