

Molecular MRI enables early and sensitive detection of brain metastases
- PMID: 22451897
- PMCID: PMC3340084
- DOI: 10.1073/pnas.1117412109
Molecular MRI enables early and sensitive detection of brain metastases
Abstract
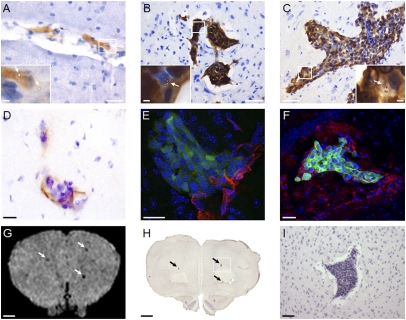
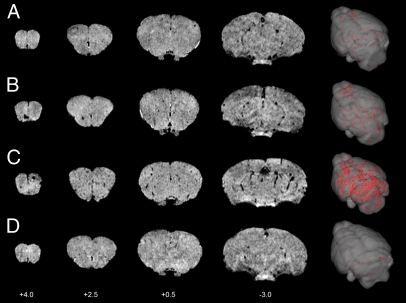
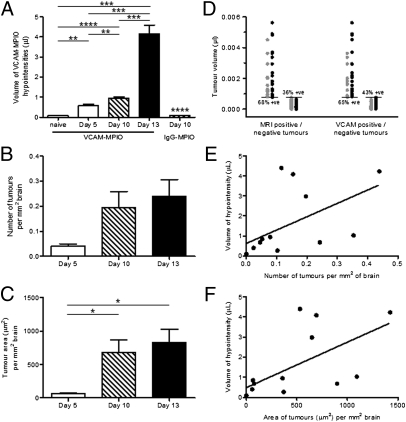
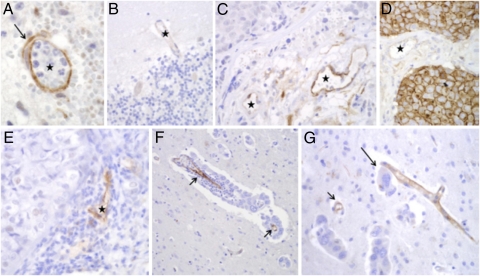
Metastasis to the brain is a leading cause of cancer mortality. The current diagnostic method of gadolinium-enhanced MRI is sensitive only to larger tumors, when therapeutic options are limited. Earlier detection of brain metastases is critical for improved treatment. We have developed a targeted MRI contrast agent based on microparticles of iron oxide that enables imaging of endothelial vascular cell adhesion molecule-1 (VCAM-1). Our objectives here were to determine whether VCAM-1 is up-regulated on vessels associated with brain metastases, and if so, whether VCAM-1-targeted MRI enables early detection of these tumors. Early up-regulation of cerebrovascular VCAM-1 expression was evident on tumor-associated vessels in two separate murine models of brain metastasis. Metastases were detectable in vivo using VCAM-1-targeted MRI 5 d after induction (<1,000 cells). At clinical imaging resolutions, this finding is likely to translate to detection at tumor volumes two to three orders of magnitude smaller (0.3-3 × 10(5) cells) than those volumes detectable clinically (10(7)-10(8) cells). VCAM-1 expression detected by MRI increased significantly (P < 0.0001) with tumor progression, and tumors showed no gadolinium enhancement. Importantly, expression of VCAM-1 was shown in human brain tissue containing both established metastases and micrometastases. Translation of this approach to the clinic could increase therapeutic options and change clinical management in a substantial number of cancer patients.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain metastases. Histology, multiplicity, surgery, and survival. Cancer. 1996;78:1781–1788. - PubMed
-
- Hochstenbag MM, Twijnstra A, Wilmink JT, Wouters EF, ten Velde GP. Asymptomatic brain metastases (BM) in small cell lung cancer (SCLC): MR-imaging is useful at initial diagnosis. J Neurooncol. 2000;48:243–248. - PubMed
-
- Suzuki K, et al. Magnetic resonance imaging and computed tomography in the diagnoses of brain metastases of lung cancer. Lung Cancer. 2004;46:357–360. - PubMed
-
- Krüger S, et al. Brain metastasis in lung cancer. Comparison of cerebral MRI and 18F-FDG-PET/CT for diagnosis in the initial staging. Nucl Med (Stuttg) 2011;50:101–106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
