

Comparative effectiveness of revascularization strategies
- PMID: 22452338
- PMCID: PMC4671393
- DOI: 10.1056/NEJMoa1110717
Comparative effectiveness of revascularization strategies
Abstract
Background: Questions persist concerning the comparative effectiveness of percutaneous coronary intervention (PCI) and coronary-artery bypass grafting (CABG). The American College of Cardiology Foundation (ACCF) and the Society of Thoracic Surgeons (STS) collaborated to compare the rates of long-term survival after PCI and CABG.
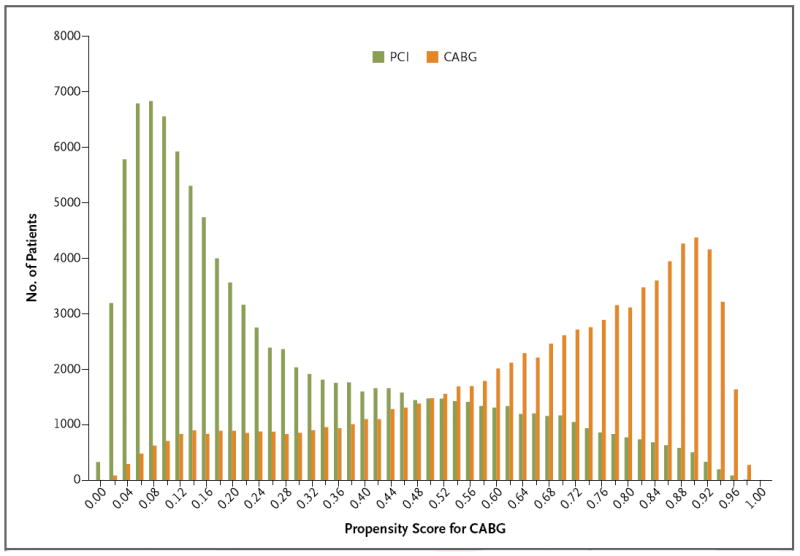
Methods: We linked the ACCF National Cardiovascular Data Registry and the STS Adult Cardiac Surgery Database to claims data from the Centers for Medicare and Medicaid Services for the years 2004 through 2008. Outcomes were compared with the use of propensity scores and inverse-probability-weighting adjustment to reduce treatment-selection bias.
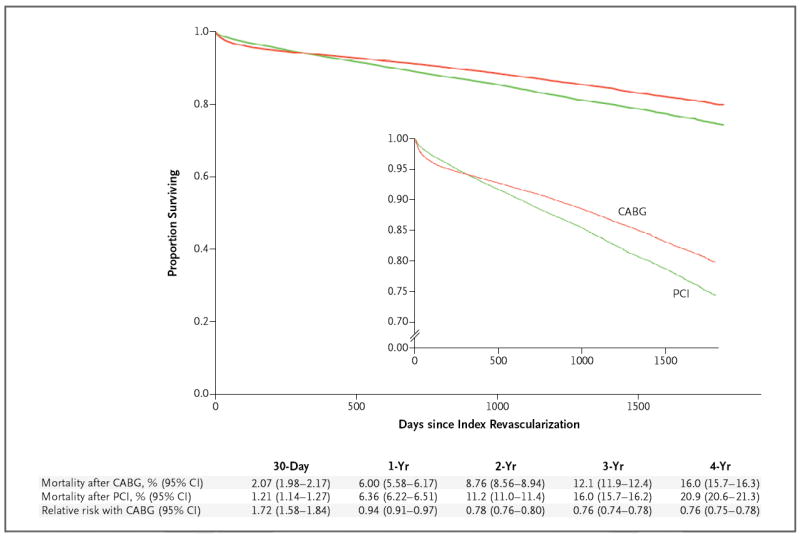
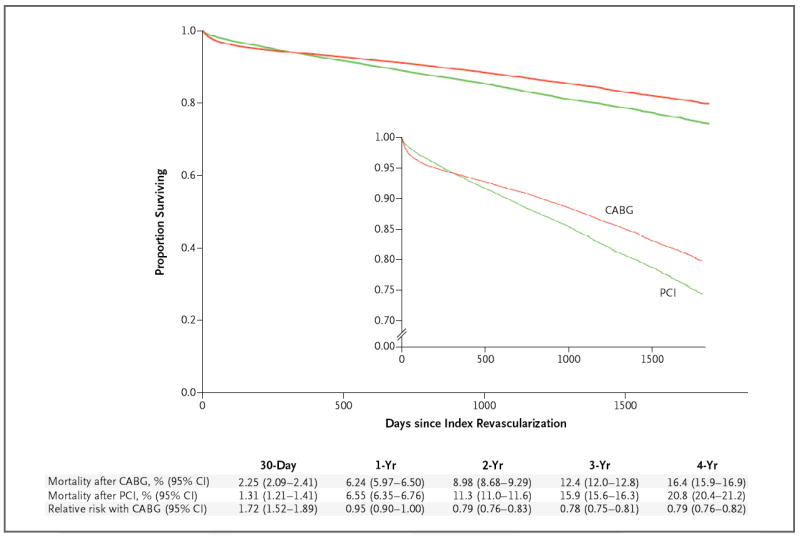
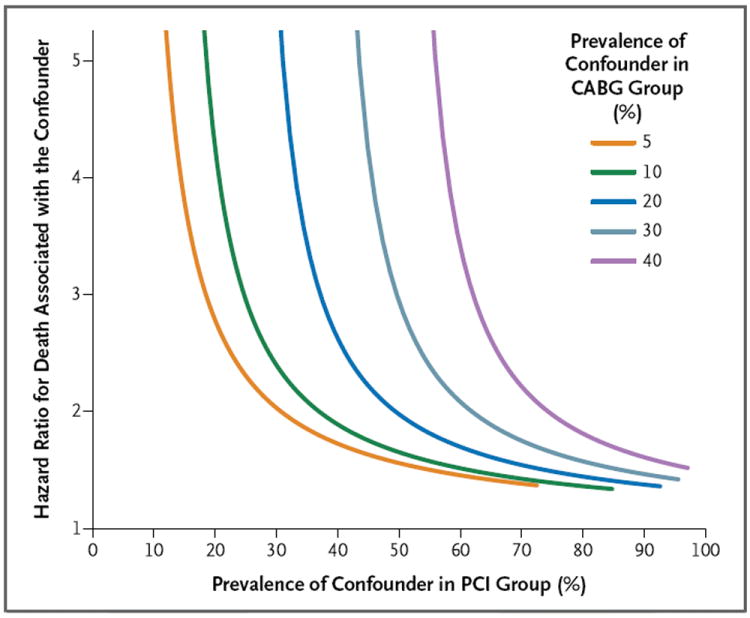
Results: Among patients 65 years of age or older who had two-vessel or three-vessel coronary artery disease without acute myocardial infarction, 86,244 underwent CABG and 103,549 underwent PCI. The median follow-up period was 2.67 years. At 1 year, there was no significant difference in adjusted mortality between the groups (6.24% in the CABG group as compared with 6.55% in the PCI group; risk ratio, 0.95; 95% confidence interval [CI], 0.90 to 1.00). At 4 years, there was lower mortality with CABG than with PCI (16.4% vs. 20.8%; risk ratio, 0.79; 95% CI, 0.76 to 0.82). Similar results were noted in multiple subgroups and with the use of several different analytic methods. Residual confounding was assessed by means of a sensitivity analysis.
Conclusions: In this observational study, we found that, among older patients with multivessel coronary disease that did not require emergency treatment, there was a long-term survival advantage among patients who underwent CABG as compared with patients who underwent PCI. (Funded by the National Heart, Lung, and Blood Institute.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Why we still need randomized trials to compare effectiveness.N Engl J Med. 2012 Apr 19;366(16):1538-40. doi: 10.1056/NEJMe1202866. Epub 2012 Mar 27. N Engl J Med. 2012. PMID: 22452337 No abstract available.
-
Comparative effectiveness of revascularization strategies.N Engl J Med. 2012 Aug 2;367(5):476; author reply 477. doi: 10.1056/NEJMc1206011. N Engl J Med. 2012. PMID: 22853023 No abstract available.
-
Comparative effectiveness of revascularization strategies.N Engl J Med. 2012 Aug 2;367(5):476-7; author reply 477. doi: 10.1056/NEJMc1206011. N Engl J Med. 2012. PMID: 22853024 No abstract available.
-
Observational studies versus randomized trials: squaring off.J Comp Eff Res. 2012 Sep;1(5):385-6. doi: 10.2217/cer.12.49. J Comp Eff Res. 2012. PMID: 24236414 No abstract available.
References
-
- Hlatky MA, Boothroyd DB, Bravata DM, et al. Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet. 2009;373:1190–7. - PubMed
-
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–72. - PubMed
-
- Rosenbaum PR, Rubin D. The central role of propensity score in observation studies for causal effects. Biometrika. 1983;70:41–55.
-
- Curtis LH, Hammill BG, Eisenstein EL, Kramer JM, Anstrom KJ. Using inverse probability-weighted estimators in comparative effectiveness analyses with observational databases. Med Care. 2007;45(Suppl 2):S103–S107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous