

Adoptive T-cell therapy using autologous tumor-infiltrating lymphocytes for metastatic melanoma: current status and future outlook
- PMID: 22453018
- PMCID: PMC3315690
- DOI: 10.1097/PPO.0b013e31824d4465
Adoptive T-cell therapy using autologous tumor-infiltrating lymphocytes for metastatic melanoma: current status and future outlook
Abstract
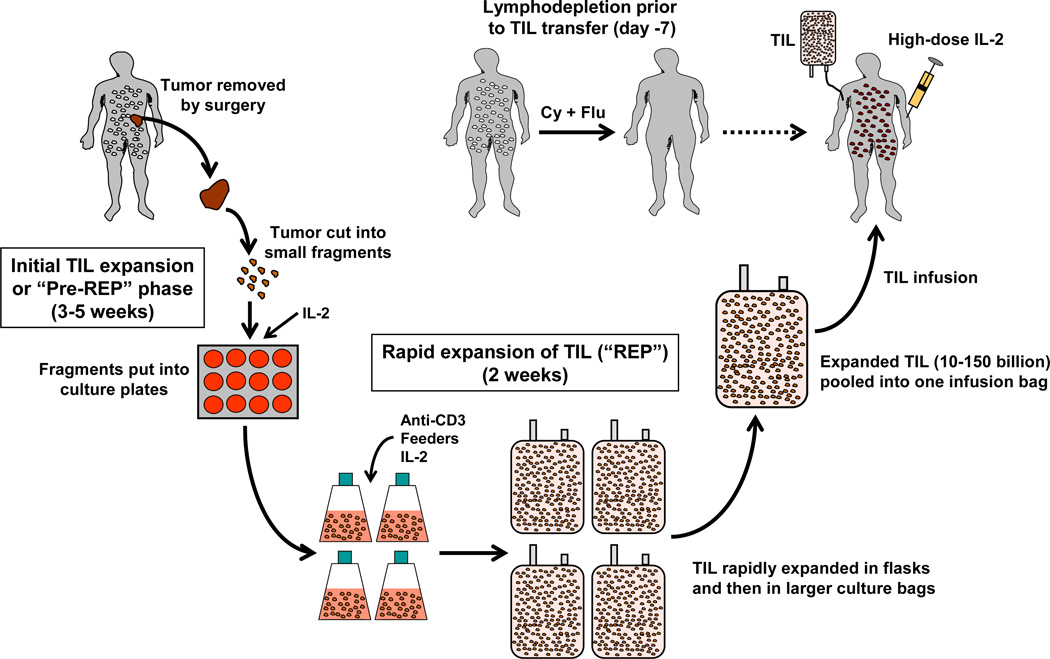
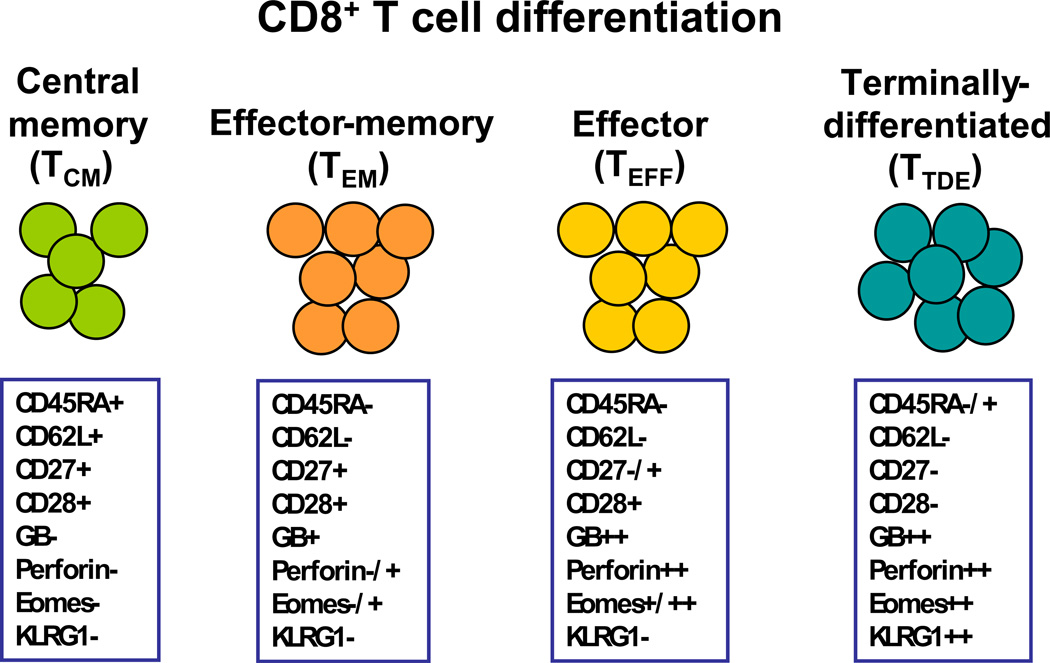
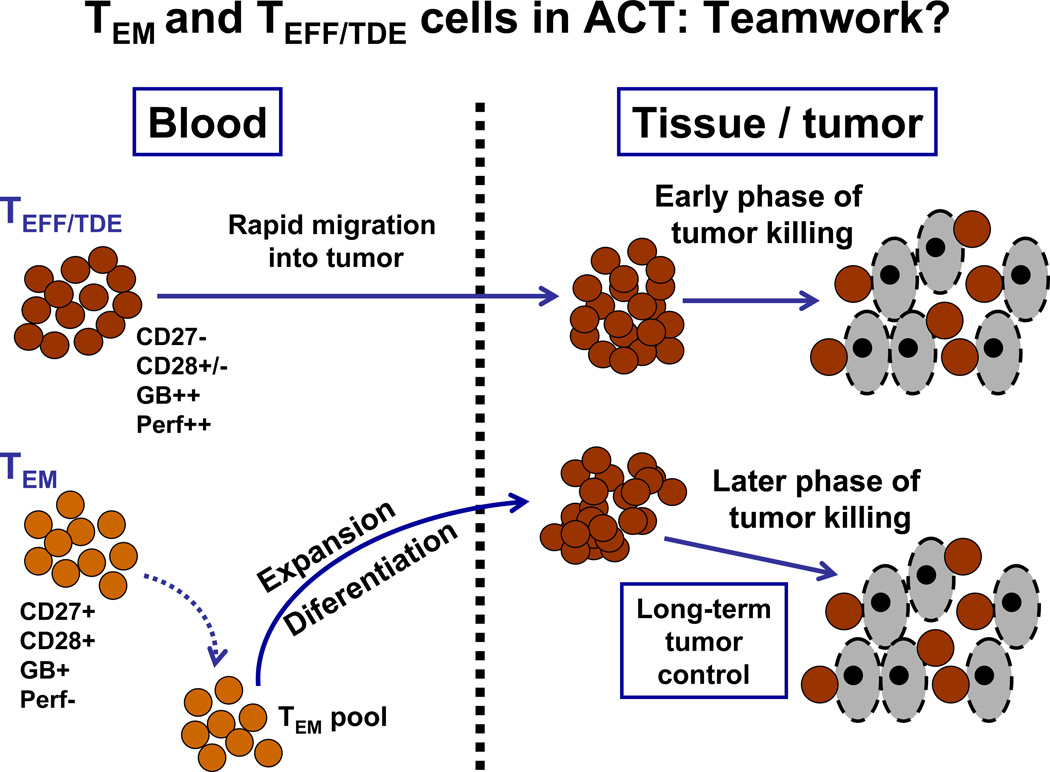
Immunotherapy using autologous T cells has emerged to be a powerful treatment option for patients with metastatic melanoma. These include the adoptive transfer of autologous tumor-infiltrating lymphocytes (TILs), T cells transduced with high-affinity T cell receptors against major tumor antigens, and T cells transduced with chimeric antigen receptors composed of hybrid immunoglobulin light chains with endodomains of T-cell signaling molecules. Among these and other options for T-cell therapy, TILs together with high-dose interleukin 2 have had the longest clinical history with multiple clinical trials in centers across the world consistently demonstrating durable clinical response rates near 50% or more. A distinct advantage of TIL therapy making it still the T-cell therapy of choice is the broad nature of the T-cell recognition against both defined and undefined tumors antigens against all possible major histocompatibility complex, rather than the single specificity and limited major histocompatibility complex coverage of the newer T cell receptors and chimeric antigen receptor transduction technologies. In the past decade, significant inroads have been made in defining the phenotypes of T cells in TIL-mediating tumor regression. CD8+ T cells are emerging to be critical, although the exact subset of CD8+ T cells exhibiting the highest clinical activity in terms of memory and effector markers is still controversial. We present a model in which both effector-memory and more differentiated effector T cells ultimately may need to cooperate to mediate long-term tumor control in responding patients. Although TIL therapy has shown great potential to treat metastatic melanoma, a number of issues have emerged that need to be addressed to bring it more into the mainstream of melanoma care. First, we have a reached the point where a pivotal phase II or phase III trial is needed in an attempt to gain regulatory approval of TILs as standard of care. Second, improvements in how we expand TILs for therapy are needed that minimize the time the T cells are in culture and improve the memory and effector characteristics of the T cells for longer persistence and enhanced anti-tumor activity in vivo. Third, there is a critical need to identify surrogate and predictive biomarkers to better select suitable patients for TIL therapy to improve response rate and duration. Overall, the outlook for TIL therapy for melanoma is very bright. We predict that TILs will indeed emerge to become an approved treatment in the upcoming years through pivotal clinical trials. Moreover, new approaches combining TILs with targeted signaling pathway drugs, such as mutant B-RAF inhibitors, and synergistic immunomodulatory interventions enhancing T-cell costimulation and preventing negative regulation should further increase therapeutic efficacy and durable complete response rates.
Figures
References
-
- Trial watch: ipilimumab success in melanoma provides boost for cancer immunotherapy. Nat Rev Drug Discov. 2010;9(8):584. - PubMed
-
- Hoos A, Ibrahim R, Korman A, Abdallah K, Berman D, Shahabi V, et al. Development of ipilimumab: contribution to a new paradigm for cancer immunotherapy. Semin Oncol. 2011;37(5):533–546. - PubMed
-
- Atkins MB, Kunkel L, Sznol M, Rosenberg SA. High-dose recombinant interleukin-2 therapy in patients with metastatic melanoma: long-term survival update. Cancer J Sci Am. 2000;6 Suppl 1:S11–S14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
