

Does a 4 diagram manual enable laypersons to operate the Laryngeal Mask Supreme®? A pilot study in the manikin
- PMID: 22453060
- PMCID: PMC3375204
- DOI: 10.1186/1757-7241-20-21
Does a 4 diagram manual enable laypersons to operate the Laryngeal Mask Supreme®? A pilot study in the manikin
Abstract
Background: Bystander resuscitation plays an important role in lifesaving cardiopulmonary resuscitation (CPR). A significant reduction in the "no-flow-time", quantitatively better chest compressions and an improved quality of ventilation can be demonstrated during CPR using supraglottic airway devices (SADs). Previous studies have demonstrated the ability of inexperienced persons to operate SADs after brief instruction. The aim of this pilot study was to determine whether an instruction manual consisting of four diagrams enables laypersons to operate a Laryngeal Mask Supreme® (LMAS) in the manikin.
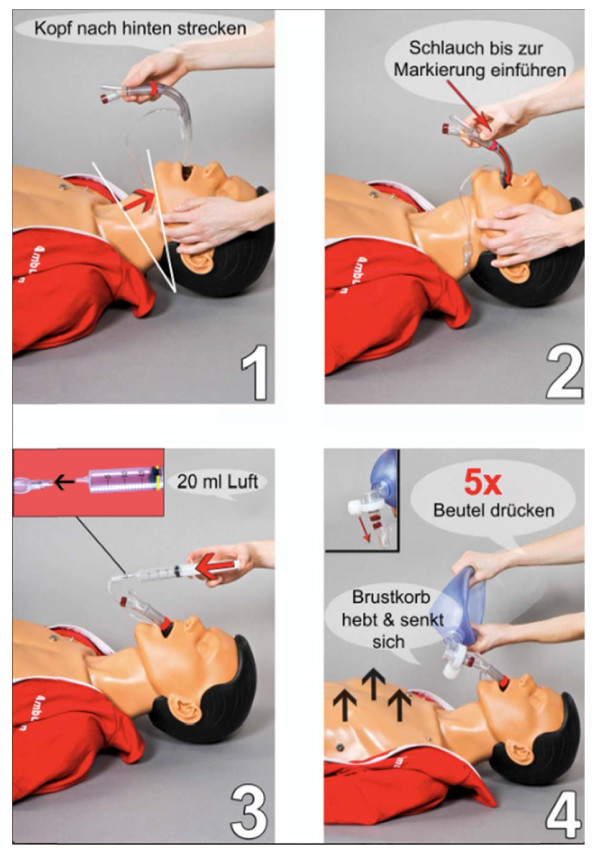
Methods: An instruction manual of four illustrations with speech bubbles displaying the correct use of the LMAS was designed. Laypersons were handed a bag containing a LMAS, a bag mask valve device (BMV), a syringe prefilled with air and the instruction sheet, and were asked to perform and ventilate the manikin as displayed. Time to ventilation was recorded and degree of success evaluated.
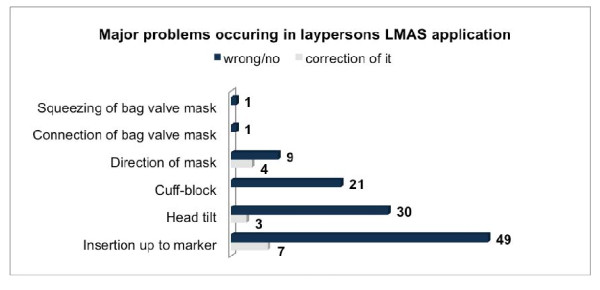
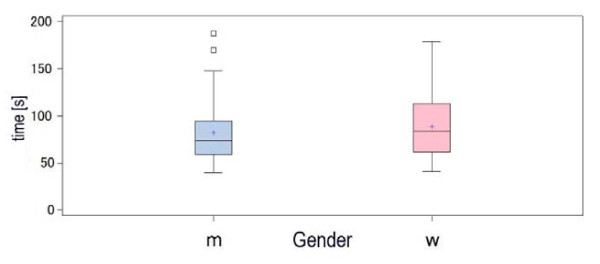
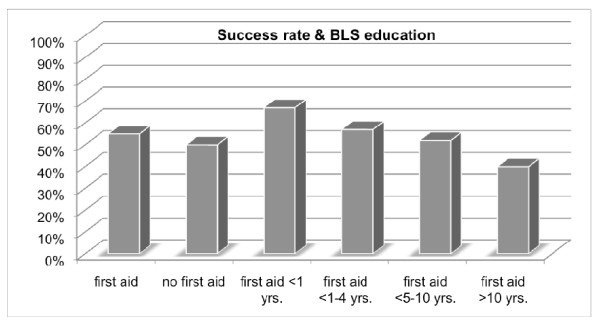
Results: A total of 150 laypersons took part. Overall 145 participants (96.7%) inserted the LMAS in the manikin in the right direction. The device was inserted inverted or twisted in 13 (8.7%) attempts. Eight (5.3%) individuals recognized this and corrected the position. Within the first 2 minutes 119 (79.3%) applicants were able to insert the LMAS and provide tidal volumes greater than 150 ml (estimated dead space). Time to insertion and first ventilation was 83.2 ± 29 s. No significant difference related to previous BLS training (P = 0.85), technical education (P = 0.07) or gender could be demonstrated (P = 0.25).
Conclusion: In manikin laypersons could insert LMAS in the correct direction after onsite instruction by a simple manual with a high success rate. This indicates some basic procedural understanding and intellectual transfer in principle. Operating errors (n = 91) were frequently not recognized and corrected (n = 77). Improvements in labeling and the quality of instructional photographs may reduce individual error and may optimize understanding.
Figures

References
-
- Handley AJ, Koster R, Monsieurs K, Perkins GD, Davies S, Bossaert L. European Resuscitation Council. European Resuscitation Council guidelines for resuscitation 2005. Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation. 2005;67(Suppl 1):S7–S23. - PubMed
-
- Wiese CH, Bartels U, Bahr J, Graf BM. Kurs Lebensrettende Sofortmaßnahmen, Überprüfung der theoretischen Kenntnisse von Teilnehmern. Notfall Rettungsmed. 2006;9:597–603. doi: 10.1007/s10049-006-0852-9. - DOI
-
- Burghofer K, Schlechtriemen T, Lackner CK. Konsequenzen aus der Altruismusforschung für die Ausbildung in Erster Hilfe. Notfall Rettungsmed. 2005;8:408–411. doi: 10.1007/s10049-005-0762-2. - DOI
-
- Baubin M. Laienreanimation ohne Mund-zu-Mund-Beatmung? Anaesthesist. 2007;56:897–898. doi: 10.1007/s00101-007-1245-2. - DOI
-
- Kreimeier U, Dirks B, Arntz HR, Bahr J, Goldschmidt P, Roessler M, Sasse M, Toursarkissian M. Stellenwert der Beatmung bei der Laienreanimation, Bestätigung der Gültigkeit der European Resuscitation Council (ERC) Guidelines 2005". Notfall Rettungsmed. 2005;11:340–343. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
