

Pharmacokinetics and tolerability of human mouse chimeric anti-CD22 monoclonal antibody in Chinese patients with CD22-positive non-Hodgkin lymphoma
- PMID: 22453099
- PMCID: PMC3361661
- DOI: 10.4161/mabs.4.2.19136
Pharmacokinetics and tolerability of human mouse chimeric anti-CD22 monoclonal antibody in Chinese patients with CD22-positive non-Hodgkin lymphoma
Abstract
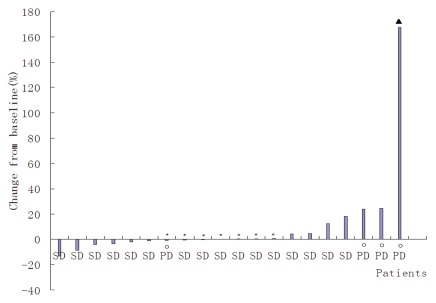
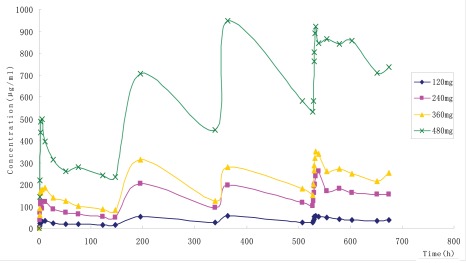
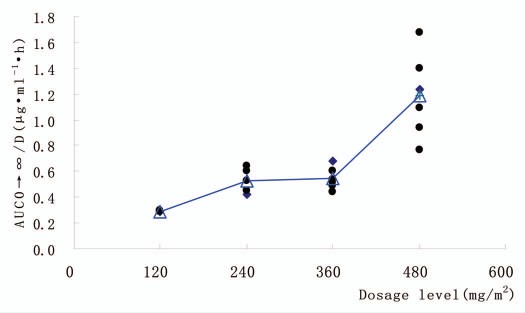
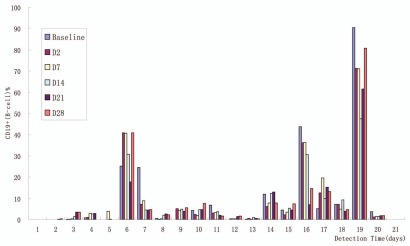
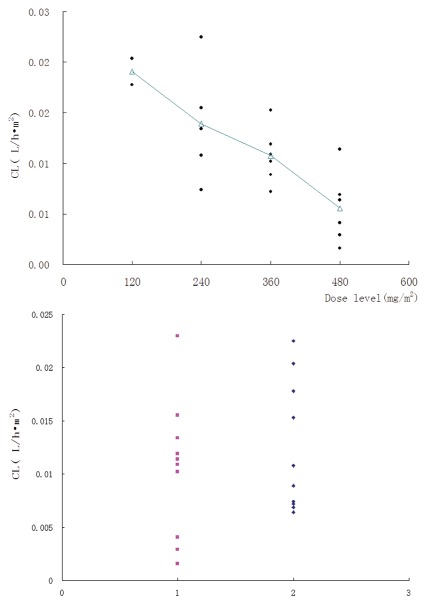
The safety and pharmacokinetics assessment of antibodies targeting CD22 (e.g., epratuzumab) have been established in western Caucasian populations, but there are no reports of the effects in Chinese populations. This dose-escalation study examines the safety, pharmacokinetics and biologic effects of multiple doses of anti-CD22 human-murine chimeric monoclonal antibody SM03 in 21 Chinese patients with CD22-positive non-Hodgkin lymphoma. Most of drug-related adverse events (AEs) were mild and reversible. Two patients experienced serious AEs (hemorrhage); one patient had grade 4 neutropenia; one patient had asymptomatic grade III prolongation of activated partial thromboplastin time (APTT). Major AEs included fever (71%), prolongation of APTT (42.8%), leukocytopenia (44.4%), alanine transaminase elevation (28.6%), elevated serum creatinine (23.8%) and injection site skin redness (14.3%). Circulating B cells transiently decreased without significant effects on T cells or immunoglobulin levels. Pharmacokinetic data revealed that mean maximum observed SM03 concentration and mean AUC from time zero to infinity increased in a dose-dependent manner up to 360 mg/m (2) SM03. Mean clearance was similar at doses ≤ 360 mg/m (2) and decreased significantly at dose 480 mg/m (2), supporting saturation of B-cell binding at 360 mg/m (2). Across all dose levels and histologies, one patient achieved partial response at 480 mg/m (2) dose; 14 patients had stable disease as best response and four patients progressed. Overall, SM03 was tolerated at doses ranging from 60-480 mg/m (2) and had potential efficacy in Chinese patients with follicular lymphoma.
Keywords: anti-CD22 monoclonal antibody; pharmacokinetics; tolerance.
Figures
References
-
- Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-Hermelink HK, Vardiman J, et al. The World Health Organization classification of neoplasms of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting—Airlie House, Virginia, November 1997. Hematol J. 2000;1:53–66. doi: 10.1038/sj.thj.6200013. - DOI - PubMed
-
- Fisher RI. Current therapeutic paradigm for the treatment of non-Hodgkin's lymphoma. Semin Oncol. 2000;27:2–8. - PubMed
-
- Gordon LI, Harrington D, Andersen J, Colgan J, Glick J, Neiman R, et al. Comparison of a second-generation combination chemotherapeutic regimen (m-BACOD) with a standard regimen (CHOP) for advanced diffuse non-Hodgkin's lymphoma. N Engl J Med. 1992;327:1342–1349. doi: 10.1056/NEJM199211053271903. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources