

Diabetic cardiomyopathy: pathophysiology and clinical features
- PMID: 22453289
- PMCID: PMC3593009
- DOI: 10.1007/s10741-012-9313-3
Diabetic cardiomyopathy: pathophysiology and clinical features
Abstract
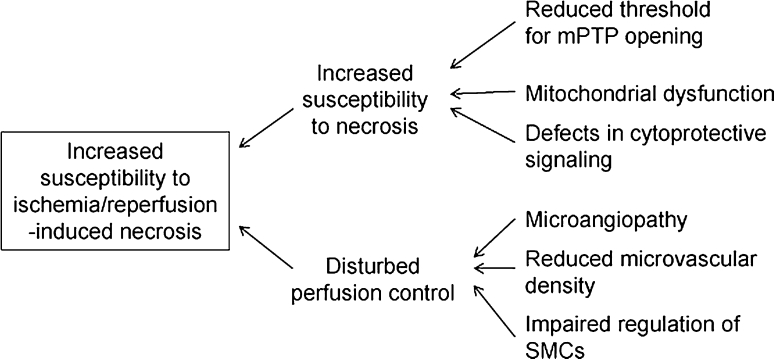
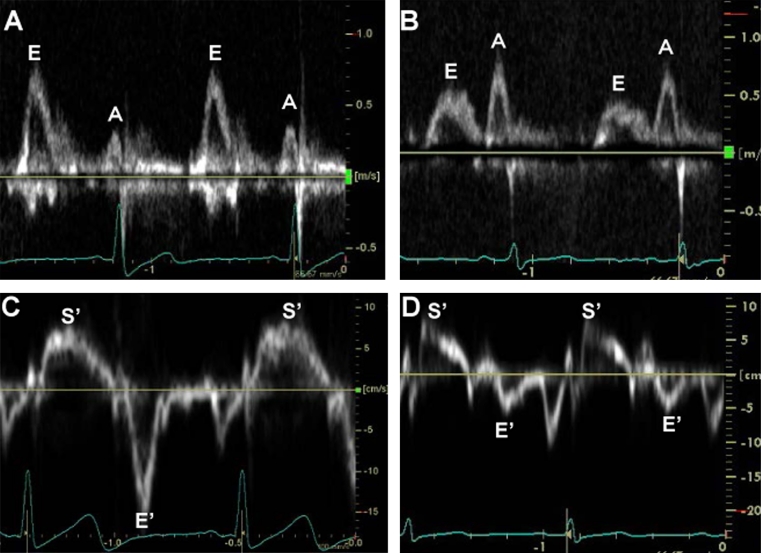
Since diabetic cardiomyopathy was first reported four decades ago, substantial information on its pathogenesis and clinical features has accumulated. In the heart, diabetes enhances fatty acid metabolism, suppresses glucose oxidation, and modifies intracellular signaling, leading to impairments in multiple steps of excitation-contraction coupling, inefficient energy production, and increased susceptibility to ischemia/reperfusion injury. Loss of normal microvessels and remodeling of the extracellular matrix are also involved in contractile dysfunction of diabetic hearts. Use of sensitive echocardiographic techniques (tissue Doppler imaging and strain rate imaging) and magnetic resonance spectroscopy enables detection of diabetic cardiomyopathy at an early stage, and a combination of the modalities allows differentiation of this type of cardiomyopathy from other organic heart diseases. Circumstantial evidence to date indicates that diabetic cardiomyopathy is a common but frequently unrecognized pathological process in asymptomatic diabetic patients. However, a strategy for prevention or treatment of diabetic cardiomyopathy to improve its prognosis has not yet been established. Here, we review both basic and clinical studies on diabetic cardiomyopathy and summarize problems remaining to be solved for improving management of this type of cardiomyopathy.
Figures


References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, Lin JK, Farzadfar F, Khang YH, Stevens GA, Rao M, Ali MK, Riley LM, Robinson CA, Ezzati M, Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Glucose) National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40. - PubMed
-
- Sobel BE. Optimizing cardiovascular outcomes in diabetes mellitus. Am J Med. 2007;120(Suppl 2):S3–S11. - PubMed
-
- Gaede P, Pedersen O. Intensive integrated therapy of type 2 diabetes: implications for long-term prognosis. Diabetes. 2004;53(Suppl 3):S39–S47. - PubMed
-
- From AM, Leibson CL, Bursi F, Redfield MM, Weston SA, Jacobsen SJ, Rodeheffer RJ, Roger VL. Diabetes in heart failure: prevalence and impact on outcome in the population. Am J Med. 2006;119:591–599. - PubMed
-
- Bell DS. Heart failure: the frequent, forgotten, and often fatal complication of diabetes. Diabetes Care. 2003;26:2433–2441. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
