

Cellular therapy with Ixmyelocel-T to treat critical limb ischemia: the randomized, double-blind, placebo-controlled RESTORE-CLI trial
- PMID: 22453769
- PMCID: PMC3369291
- DOI: 10.1038/mt.2012.52
Cellular therapy with Ixmyelocel-T to treat critical limb ischemia: the randomized, double-blind, placebo-controlled RESTORE-CLI trial
Abstract
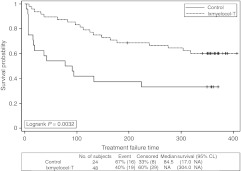
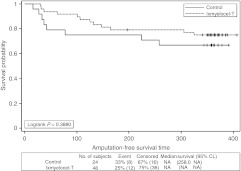
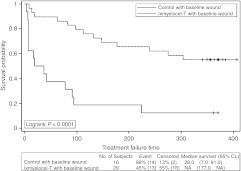
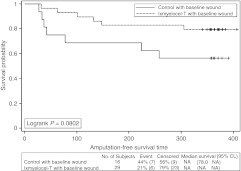
Ixmyelocel-T is a patient-specific, expanded, multicellular therapy evaluated in patients with lower extremity critical limb ischemia (CLI) with no options for revascularization. This randomized, double-blind, placebo-controlled, phase 2 trial (RESTORE-CLI) compared the efficacy and safety of intramuscular injections of ixmyelocel-T with placebo. Patients received one-time injections over 20 locations in a single leg and were followed for 12 months. Safety assessments included occurrence of adverse events. Efficacy assessments included time to first occurrence of treatment failure (TTF; major amputation of injected leg; all-cause mortality; doubling of total wound surface area from baseline; de novo gangrene) and amputation-free survival (AFS; major amputation of injected leg; all-cause mortality). A total of 77 patients underwent bone marrow or sham aspiration; 72 patients received ixmyelocel-T (48 patients) or placebo (24 patients). Adverse event rates were similar. Ixmyelocel-T treatment led to a significantly prolonged TTF (P = 0.0032, logrank test). AFS had a clinically meaningful 32% reduction in event rate that was not statistically significant (P = 0.3880, logrank test). Treatment effect in post hoc analyses of patients with baseline wounds was more pronounced (TTF: P < 0.0001, AFS: P = 0.0802, logrank test). Ixmyelocel-T treatment was well tolerated and may offer a potential new treatment option.
Figures

References
-
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, American Association for Vascular Surgery; Society for Vascular Surgery; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease; American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; Vascular Disease Foundation. (2006) et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 113:e463–e654. - PubMed
-
- Allison MA, Ho E, Denenberg JO, Langer RD, Newman AB, Fabsitz RR.et al. (2007Ethnic-specific prevalence of peripheral arterial disease in the United States Am J Prev Med 32328–333. - PubMed
-
- Ostchega Y, Paulose-Ram R, Dillon CF, Gu Q., and, Hughes JP. Prevalence of peripheral arterial disease and risk factors in persons aged 60 and older: data from the National Health and Nutrition Examination Survey 1999–2004. J Am Geriatr Soc. 2007;55:583–589. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–S75. - PubMed
-
- Falluji N., and, Mukherjee D. Contemporary management of infrapopliteal peripheral arterial disease. Angiology. 2011;62:490–499. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
