

Efficacy of ethinylestradiol 20 μg/drospirenone 3 mg in a flexible extended regimen in women with moderate-to-severe primary dysmenorrhoea: an open-label, multicentre, randomised, controlled study
- PMID: 22454006
- PMCID: PMC3353877
- DOI: 10.1136/jfprhc-2011-100225
Efficacy of ethinylestradiol 20 μg/drospirenone 3 mg in a flexible extended regimen in women with moderate-to-severe primary dysmenorrhoea: an open-label, multicentre, randomised, controlled study
Abstract
Objectives: The aim of this Phase III, multicentre, open-label, randomised study was to compare the efficacy and safety of ethinylestradiol (EE)/drospirenone (DRSP) in a new flexible extended regimen that allowed the management of intracyclic (breakthrough) bleeding (MIB) with that of EE/DRSP in a conventional 28-day regimen in women with moderate-to-severe primary dysmenorrhoea.
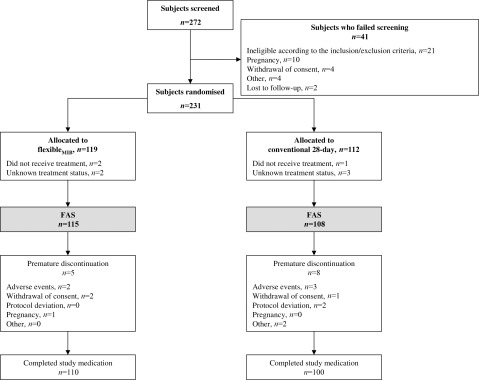
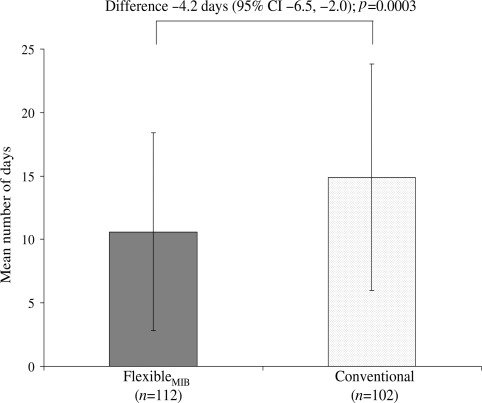
Methods: Women (aged 18-40 years) with moderate-to-severe primary dysmenorrhoea-related pain received a flexible extended regimen with MIB (flexible(MIB); minimum 24, maximum 120 days of continuous tablet intake for a flexible number of cycles to reach a treatment duration of at least 140 days with 4-day breaks between cycles) or a conventional 28-day regimen (24 active and four placebo tablets for five cycles) of EE/DRSP. The primary outcome was the number of days with dysmenorrhoeic pain over 140 days. Secondary outcomes included other dysmenorrhoea-related pain outcomes, bleeding profile, satisfaction and safety.
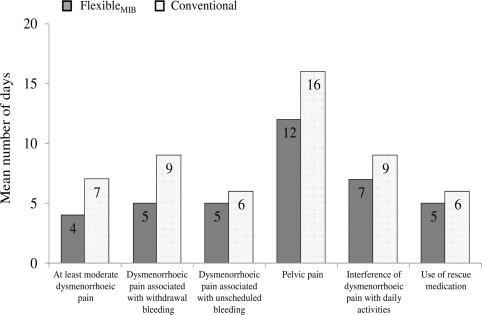
Results: Overall, 223 patients received study medication. There were significantly fewer days with dysmenorrhoeic pain with the flexible(MIB) regimen than the conventional regimen (difference -4.2 days, 95% CI -6.5 to -2.0; p=0.0003), as well as considerably fewer days with at least moderate dysmenorrhoeic pain (difference -2.5 days, 95% CI -3.7 to -1.3), dysmenorrhoeic pain that interfered with daily activities (difference -2.2 days, 95% CI -4.2 to -0.1) and pelvic pain (difference -3.4 days, 95% CI -5.9 to -0.9). Adverse events were similar with both regimens.
Conclusions: Compared with the conventional regimen, the flexible extended regimen of EE/DRSP with MIB was associated with a significantly greater reduction in days with dysmenorrhoeic pain in women with moderate-to-severe primary dysmenorrhoea. The flexible(MIB) regimen was also associated with greater improvements in dysmenorrhea according to the Clinical Global Impression rating scale and was generally well tolerated.
Conflict of interest statement
Figures
References
-
- Coco AS. Primary dysmenorrhea. Am Fam Physician 1999;60:489–496 - PubMed
-
- French L. Dysmenorrhea. Am Fam Physician 2005;71:285–291 - PubMed
-
- Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol 2006;108:428–441 - PubMed
-
- Davis AR, Westhoff CL. Primary dysmenorrhea in adolescent girls and treatment with oral contraceptives. J Pediatr Adolesc Gynecol 2001;14:3–8 - PubMed
-
- Bjorkman DJ. Current status of nonsteroidal anti-inflammatory drug (NSAID) use in the United States: risk factors and frequency of complications. Am J Med 1999;107:3S–8S; discussion 8S - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical