

Association of AKI with mortality and complications in hospitalized patients with cirrhosis
- PMID: 22454364
- PMCID: PMC3390443
- DOI: 10.1002/hep.25735
Association of AKI with mortality and complications in hospitalized patients with cirrhosis
Abstract
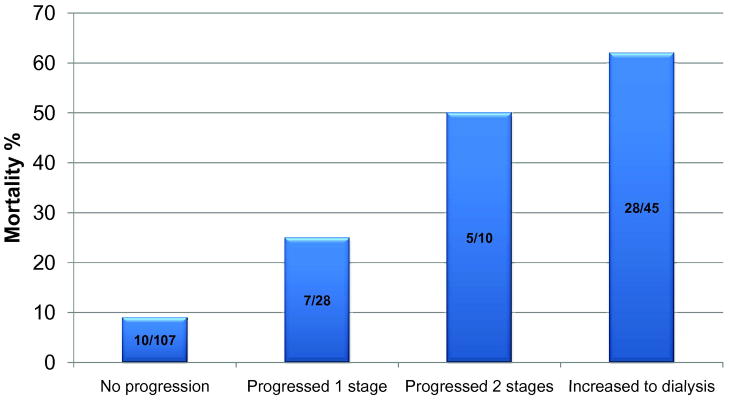
Acute kidney injury (AKI) is a common and devastating complication in patients with cirrhosis. However, the definitions of AKI employed in studies involving patients with cirrhosis have not been standardized, lack sensitivity, and are often limited to narrow clinical settings. We conducted a multicenter, prospective observational cohort study of patients with cirrhosis and AKI, drawn from multiple hospital wards, utilizing the modern acute kidney injury network (AKIN) definition and assessed the association between AKI severity and progression with in-hospital mortality. Of the 192 patients who were enrolled and included in the study, 85 (44%) progressed to a higher AKIN stage after initially fulfilling AKI criteria. Patients achieved a peak severity of AKIN stage 1, 26%, stage 2, 24%, and stage 3, 49%. The incidence of mortality, general medical events (bacteremia, pneumonia, urinary tract infection), and cirrhosis-specific complications (ascites, encephalopathy, spontaneous bacterial peritonitis) increased with severity of AKI. Progression was significantly more common and peak AKI stage higher in nonsurvivors than survivors (P < 0.0001). After adjusting for baseline renal function, demographics, and critical hospital- and cirrhosis-associated variables, progression of AKI was independently associated with mortality (adjusted odds ratio = 3.8, 95% confidence interval 1.3-11.1).
Conclusion: AKI, as defined by AKIN criteria, in patients with cirrhosis is frequently progressive and severe and is independently associated with mortality in a stage-dependent fashion. Methods for earlier diagnosis of AKI and its progression may result in improved outcomes by facilitating targeted and timely treatment of AKI.
Copyright © 2012 American Association for the Study of Liver Diseases.
Figures


Comment in
-
Acute kidney injury in cirrhosis: a changing spectrum.Hepatology. 2013 Feb;57(2):435-7. doi: 10.1002/hep.26003. Hepatology. 2013. PMID: 22886711 No abstract available.
References
-
- du Cheyron D, Bouchet B, Parienti JJ, Ramakers M, Charbonneau P. The attributable mortality of acute renal failure in critically ill patients with liver cirrhosis. Intensive Care Med. 2005;31:1693–1699. - PubMed
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48(6):2064–2077. - PubMed
-
- Bern MM. Hepatorenal syndrome: study of clinical characteristics in a large series. South Med J. 1973;66(7):775–778. - PubMed
-
- Al Sibae MR, Cappell MS. Accuracy of MELD scores in predicting mortality in decompensated cirrhosis from variceal bleeding, hepatorenal syndrome, alcoholic hepatitis, or acute liver failure as well as mortality after non-transplant surgery or TIPS. Dig Dis Sci. 2011;56(4):977–987. - PubMed
-
- Arroyo V, Ginés P, Gerbes AL, Dudley FJ, Gentilini P, Laffi G, et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. International Ascites Club Hepatology. 1996;23(1):164–176. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical