

Indocyanine green angiography guided management of vogt-koyanagi-harada disease
- PMID: 22454746
- PMCID: PMC3306120
Indocyanine green angiography guided management of vogt-koyanagi-harada disease
Abstract
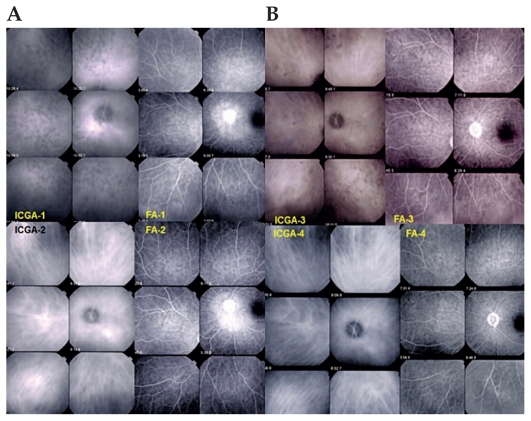
Purpose: To report the management of Vogt-Koyanagi-Harada (VKH) disease based on indocyanine green angiography (ICGA).
Methods: VKH patients with acute episodes of inflammation (inaugural or recurrent) who had received standard ICGA-guided care were studied retrospectively. Standard of care included high dose systemic corticosteroids at presentation and close ICGA follow-up with addition of immunosuppressive agents and/or intensification of ongoing therapy when recurrent choroidal lesions were detected by ICGA. Visual acuity, number of subclinical recurrences, type and duration of therapy, proportion of quiescent patients after therapy, and ICGA findings were recorded.
Results: Nine patients including 8 female and one male subject were studied. Five patients had inaugural disease and 4 presented with recurrent acute episodes. Visual acuity increased from 0.86±0.36 to 1.14±0.34 in the right eyes, and from 0.77±0.34 to 1.05±0.33 in the left eyes. The number of ICGA-detected occult choroidal recurrences amounted to 13. Mean duration of treatment was 30.1±34.6 months leading to recurrence-free status after discontinuation of therapy in 6 cases with mean duration of 29.5 months.
Conclusion: Continuous monitoring and aggressive therapy guided by ICGA in VKH disease prolongs treatment as compared to textbook guidelines but offers the prospect of reaching inflammation-free status after discontinuation of therapy. Zero tolerance to subclinical choroidal inflammation avoids irremediable evolution towards sunset glow fundus in patients treated early after the initial acute inflammatory attack.
Keywords: Indocyanine Green Angiography; Therapy; Vogt-Koyanagi-Harada Disease.
Figures
References
-
- Bouchenaki N, Herbort CP. Stromal choroiditis. In: Pleyer U, Mondino B, editors. Essentials in Ophthalmology: Uveitis and Immunological Disorders. 1st ed. Berlin, Heidelberg, New York: Springer; 2004. pp. 234–253.
-
- Sugita S, Takase H, Taguchi C, Imai Y, Kamoi K, Kawaguchi T, et al. Ocular infiltrating CD4+ T cells from patients with Vogt-Koyanagi-Harada disease recognize human melanocyte antigens. Invest Ophthalmol Vis Sci. 2006;47:2547–2554. - PubMed
-
- Damico FM, Cunha-Neto E, Goldberg AC, Iwai LK, Marin ML, Hammer J, et al. T-cell recognition and cytokine profile induced by melanocyte epitopes in patients with HLA-DRB1*0405-positive and -negative Vogt-Koyanagi-Harada uveitis. Invest Ophthalmol Vis Sci. 2005;46:2465–2471. - PubMed
-
- Sonoda S, Nakao K, Ohba N. Extensive chorioretinal atrophy in Vogt-Koyanagi-Harada disease. Jpn J Ophthalmol. 1999;43:113–119. - PubMed
-
- Rao NA. Treatment of Vogt-Koyanagi-Harada disease by corticosteroids and immunosuppressive agents. Ocul Immunol Inflamm. 2006;14:71–72. - PubMed
LinkOut - more resources
Full Text Sources