

Incidence and risk factors for acute kidney injury in HIV Infection
- PMID: 22456100
- PMCID: PMC3362304
- DOI: 10.1159/000337151
Incidence and risk factors for acute kidney injury in HIV Infection
Abstract
Background/aims: Although HIV-infected persons are at higher risk for acute kidney injury (AKI) during hospitalization compared with their uninfected counterparts, risk factors for AKI are not well-defined. We aimed to describe the evolving incidence of AKI among HIV-infected individuals and to identify important AKI risk factors.
Methods: We conducted a prospective cohort study of 56,823 HIV-infected persons in the Department of Veterans Affairs Clinical Case Registry. Outcomes were: AKI (acute in-hospital serum creatinine increase of ≥0.3 mg/dl, or a relative increase by 50% or greater), and dialysis-requiring AKI. We used proportional hazards regressions to identify risk factors.
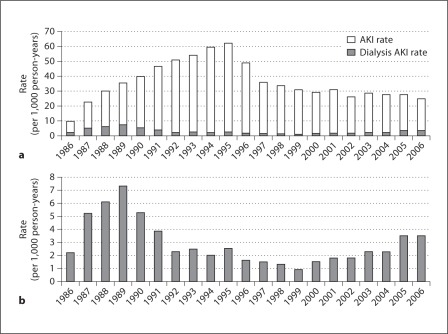
Results: From its peak in 1995 at 62 per 1,000 person-years, the incidence of AKI declined after the introduction of highly active antiretroviral therapy (HAART) in 1996 to a low point of 25 per 1,000 person-years in 2006. Incidence of dialysis-requiring AKI declined in the early 1990s, but doubled between 2000 and 2006. Using multivariate proportional hazard regression, we identified the following strong risk factors for AKI: chronic kidney disease (eGFR <60 ml/min/1.73 m(2)) (5.38, 95% CI: 5.11-5.67), proteinuria (1.78, 1.70-1.87), low serum albumin (<3.7 mg/dl) (5.24, 4.82-5.71), low body mass index (<18.5 kg/m(2)) (1.69, 1.54-1.86), cardiovascular disease (1.77, 1.66-1.89), low CD4 count (<200 cells/mm(3)) (2.54, 2.33-2.77), and high viral load (≥100,000 copies/ml) (2.51, 2.28-2.75). In addition, there was substantial heterogeneity in the strengths of risk factors for dialysis-requiring AKI before and after the introduction of HAART.
Conclusions: Although AKI incidence has decreased during the HAART era, it remains common in HIV-infected persons and appears attributable to both kidney- and HIV-related factors.
Copyright © 2012 S. Karger AG, Basel.
Figures
References
-
- Lameire N, Van Biesen W, Vanholder R. The changing epidemiology of acute renal failure. Nat Clin Pract Nephrol. 2006;2:364–377. - PubMed
-
- Lattanzio MR, Kopyt NP. Acute kidney injury: New concepts in definition, diagnosis, pathophysiology, and treatment. J Am Osteopath Assoc. 2009;109:13–19. - PubMed
-
- Wyatt CM, Arons RR, Klotman PE, Klotman ME. Acute renal failure in hospitalized patients with HIV: risk factors and impact on in-hospital mortality. AIDS. 2006;20:561–565. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
