

Mutations in cytoplasmic loops of the KCNQ1 channel and the risk of life-threatening events: implications for mutation-specific response to β-blocker therapy in type 1 long-QT syndrome
- PMID: 22456477
- PMCID: PMC3690492
- DOI: 10.1161/CIRCULATIONAHA.111.048041
Mutations in cytoplasmic loops of the KCNQ1 channel and the risk of life-threatening events: implications for mutation-specific response to β-blocker therapy in type 1 long-QT syndrome
Abstract
Background: β-Adrenergic stimulation is the main trigger for cardiac events in type 1 long-QT syndrome (LQT1). We evaluated a possible association between ion channel response to β-adrenergic stimulation and clinical response to β-blocker therapy according to mutation location.
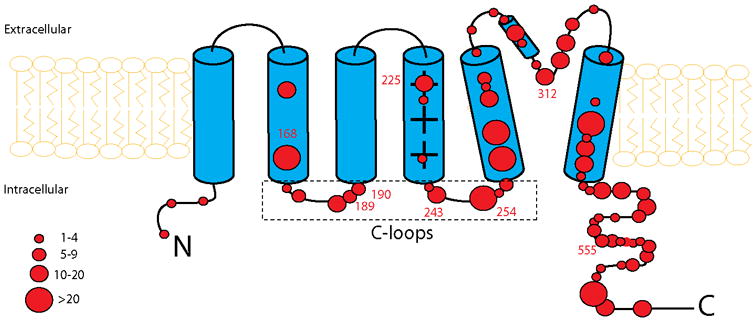
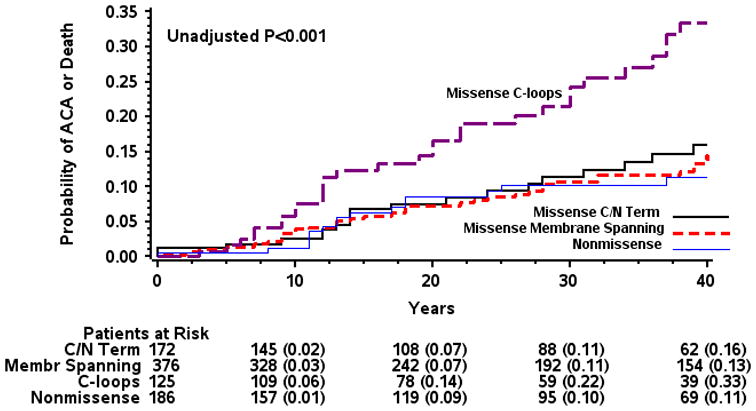
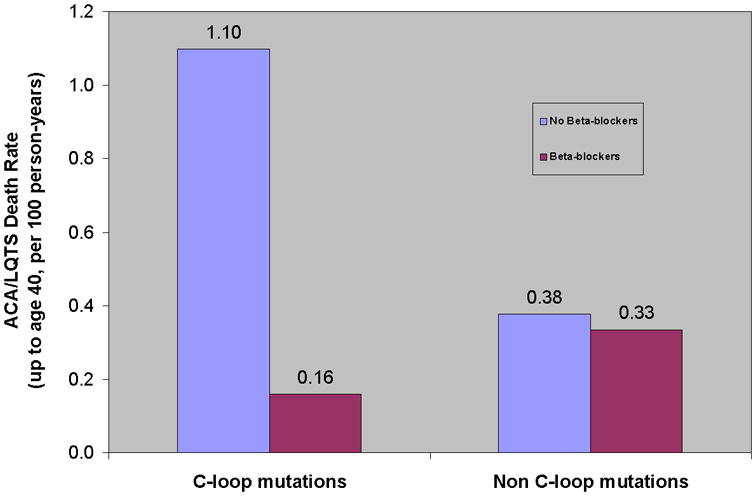
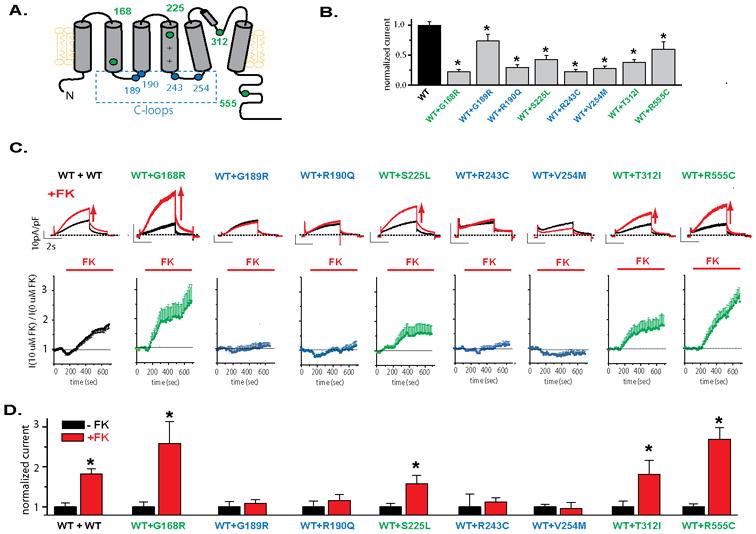
Methods and results: The study sample comprised 860 patients with genetically confirmed mutations in the KCNQ1 channel. Patients were categorized into carriers of missense mutations located in the cytoplasmic loops (C loops), membrane-spanning domain, C/N terminus, and nonmissense mutations. There were 27 aborted cardiac arrest and 78 sudden cardiac death events from birth through 40 years of age. After multivariable adjustment for clinical factors, the presence of C-loop mutations was associated with the highest risk for aborted cardiac arrest or sudden cardiac death (hazard ratio versus nonmissense mutations=2.75; 95% confidence interval, 1.29-5.86; P=0.009). β-Blocker therapy was associated with a significantly greater reduction in the risk of aborted cardiac arrest or sudden cardiac death among patients with C-loop mutations than among all other patients (hazard ratio=0.12; 95% confidence interval, 0.02-0.73; P=0.02; and hazard ratio=0.82; 95% confidence interval, 0.31-2.13; P=0.68, respectively; P for interaction=0.04). Cellular expression studies showed that membrane spanning and C-loop mutations produced a similar decrease in current, but only C-loop mutations showed a pronounced reduction in channel activation in response to β-adrenergic stimulation.
Conclusions: Patients with C-loop missense mutations in the KCNQ1 channel exhibit a high risk for life-threatening events and derive a pronounced benefit from treatment with β-blockers. Reduced channel activation after sympathetic activation can explain the increased clinical risk and response to therapy in patients with C-loop mutations.
Figures
Comment in
-
Meandering pathway leading from genotyping to personalized management of long-QT syndrome.Circulation. 2012 Apr 24;125(16):1961-3. doi: 10.1161/CIRCULATIONAHA.112.102293. Epub 2012 Mar 28. Circulation. 2012. PMID: 22456476 No abstract available.
References
-
- Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol. 2008;51:2291–2300. - PubMed
-
- Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C, Denjoy I, Guicheney P, Breithardt G, Keating MT, Towbin JA, Beggs AH, Brink P, Wilde AA, Toivonen L, Zareba W, Robinson JL, Timothy KW, Corfield V, Wattanasirichaigoon D, Corbett C, Haverkamp W, Schulze-Bahr E, Lehmann MH, Schwartz K, Coumel P, Bloise R. Genotype-phenotype correlation in the long-QT syndrome: Gene-specific triggers for life-threatening arrhythmias. Circulation. 2001;103:89–95. - PubMed
-
- Walsh KB, Kass RS. Regulation of a heart potassium channel by protein kinase A and C. Science. 1988;242:67–69. - PubMed
-
- Marx SO, Kurokawa J, Reiken S, Motoike H, D'Armiento J, Marks AR, Kass RS. Requirement of a macromolecular signaling complex for beta adrenergic receptor modulation of the KCNQ1-KCNE1 potassium channel. Science. 2002;295:496–499. - PubMed
-
- Shimizu W, Antzelevitch C. Differential effects of beta-adrenergic agonists and antagonists in LQT1, LQT2 and LQT3 models of the long QT syndrome. J Am Coll Cardiol. 2000;35:778–786. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
